

Abstract
Distinct from conventional Foxp3+ regulatory T cells (Tregs), T-bet+ Tregs represent a stable subset of immunosuppressive T cells characterized by co-expression of the transcription factors (TFs) Foxp3 and T-bet. Given that Tregs were also reported to co-express Foxp3 together with effector T cell TFs such as GATA3, or RORγt, we propose the term hybrid Tregs (hTregs) to distinguish between these Tregs that co-express Foxp3 together with effector T cell TFs from conventional Foxp3+ Tregs. Therefore, this review will focus on hTreg cells, a specific subset of CD4+ T cells, and discuss the different types of hTregs with particular emphasis on T-bet+ hTregs. T-bet+ hTregs exhibit unique features including IFN-γ production, high expression of immune checkpoints (PD-1, CTLA-4, GITR, OX40, TIGIT), and chemokine receptors (CXCR3, CCR5). Through secretion of IL-10, TGF-β and IFN-γ, T-bet+ hTregs modulate both innate and adaptive immune responses within the tumor microenvironment (TME). Their high expression of CD73 contributes to adenosine-mediated immunosuppression, while CXCR3 and CCR5 facilitate their recruitment to inflammatory sites. T-bet+ hTregs were reported to accumulate in multiple human cancers, including lung, ovarian, and colorectal carcinomas. Despite these advancements, the function of hTregs in diseases such as cancer remains poorly understood, and requires further investigations. For instance, some studies suggest T-bet+ hTregs to be anti-inflammatory due to their production of IL-10, TGF-β, and superior suppressive capacity compared to conventional Tregs. Yet, other studies have reported that T-bet+ hTregs exhibit enhanced proinflammatory functions in colitis and other pathologies. We will then highlight current known mechanisms that promote the differentiation and functions of T-bet+ hTregs in cancer. Lastly, we will discuss the advancements and opportunities for therapeutic targeting of T-bet+ hTregs in cancer immunotherapy.
1 Introduction
The tumor microenvironment (TME) comprises of cancerous cells, and a diverse array and interaction of non-cancerous cells, including stromal and immune cells (1). Within such an ecosystem, the diversity of cell-cell interactions, cellular synapses, and secretome within the TME define the fate of tumor progression, metastasis rates, and treatment outcomes in patients (2–4). Tumor infiltrated T cells (TILs) exhibit substantial heterogeneity in their phenotypes, functional states, and spatial distributions within tumors (5, 6). Regulatory T cells (Tregs) that express the transcription factor Foxp3 are among the most abundant T cell subsets within the TME (7). Similar to conventional T cells, Tregs respond to T cell antigen receptor (TCR) stimulation by transitioning from a resting state to a more suppressive effector Treg (eTreg) phenotype (8). Although, the immunosuppressive capacity of Tregs play an indispensable role in maintaining tolerance and immune homeostasis, it suppresses antitumor immune responses in the TME (7, 9). Currently, one of the challenges in the Treg field is successfully manipulating Tregs in cancer without triggering autoimmunity. However, Tregs should not be considered as a homogeneous population. During the last decade, different hybrid subsets of Tregs such as Th1-like Tregs and Th17-like Tregs have been discovered in various human and mouse diseases (10). Nevertheless, the terms “Th1-like” or “Th17-like” Tregs, which have been widely used do not properly describe these unique cells. For instance, in cancer, T-bet+ Tregs exhibit characteristics that more closely resemble conventional Tregs than Th1 cells. Likewise, RORγt+ Tregs and GATA3+ Tregs display properties that are similar to conventional Tregs than their helper T cell counterpart. Simply, these cells are not equivalent to the helper T cells and only partially share certain characteristics. We propose the term ‘hybrid Tregs’ to reflect their expression of two T cell lineage master transcription factors that regulate T cell fate and differentiation. Henceforth, we will use the term hybrid Tregs (hTregs) to refer to these subsets of regulatory T cells. Notably, hybrid subsets of Tregs are functionally different, compared to conventional Foxp3+ Tregs. For example, while conventional Tregs broadly suppress diverse immune responses, T-bet+ hTregs specifically target and suppress Th1-type immune responses and associated inflammation.
T-bet+ hTregs are defined by the co-expression of the Th1 cell transcription factor T-box transcription factor TBX21 (T-bet) and the Treg signature transcription factor Foxp3 (11). A significant accumulation of T-bet+ hTregs is reported in several tumors including oropharyngeal squamous cell carcinoma and lung carcinoma (11, 12). T-bet+ hTregs exhibit high resistance to oxidative stress, which may contribute to their accumulation in tumor tissues (13). In addition, T-bet+ hTregs primarily execute their immunosuppressive characteristics by dampening type 1 immune responses including the activation of Th1 cells and cytotoxic CD8+ T cells which are essential for antitumor immunity and defense against intracellular pathogens (14). Despite their immunosuppressive functions and abundance within the TME, the precise contribution of T-bet+ hTregs to tumor progression remains poorly understood. Given that they share features with both Tregs and Th1 cells, T-bet+ hTregs were suggested to influence the tumor immune landscape by suppressing antitumor immunity, yet their exact role in promoting or inhibiting tumor growth, metastasis, and response to immunotherapy remains less understood. In this review, we aim to shed light on the possible functional mechanisms of T-bet+ hTregs by exploring their resemblance to conventional Tregs.
2 Plasticity of Tregs and hybrid Tregs within tumors
Given the central role of conventional Tregs in regulating and maintaining immune homeostasis, they require steady and robust suppressor functions. Nonetheless, Tregs have been shown to exhibit substantial plasticity which enables them to effectively suppress a wide range of immune responses. Although this flexibility is driven by intrinsic molecular signaling pathways, such as the PI3K/AKT pathway, the activation of these pathways is also influenced by the surrounding environment of the Tregs, including various cytokines and metabolic factors (15, 16). This adaptability gives rise to specialized subsets of Tregs called hybrid Tregs which further refine immune regulation. Hybrid Tregs co-express lineage-defining transcription factors typically associated with other T helper (Th) subsets, such as T-bet (Th1), GATA3 (Th2), RORγt (Th17), and Bcl6 (Tfh) (16). These hybrid populations are thought to be crucial for suppressing their corresponding effector T cell counterparts. For instance, RORγt+ hTregs play a role in regulating Th17 responses in the gut (17).
2.1 T-bet+ hTregs
The frequency of T-bet+ hTregs among CD4+ T cells in the peripheral blood of healthy humans has been reported to be less than 2% (~6 cells/µL). In contrast, their frequency among memory Tregs has been reported to be approximately 40% in rheumatoid arthritis (18). Under specific inflammatory conditions T-bet+ hTregs differentiate from Tregs and their presence in different disease including Type 1 diabetes, Rheumatoid arthritis, and cancer have been reported (18, 19). Like conventional Tregs, T-bet+ hTregs also express Foxp3 and Helios, but in addition, they upregulate T-bet and CXCR3 (20). In settings with elevated cytokines including IFN-γ, interleukin-27 (IL-27) and IL-12, conventional Tregs sense and upregulate T-bet, as well as secrete IFN-γ and TGF-β, and exhibit other Th1-related markers such as CXCR3 and CCR5 (13, 19, 21–23). Table 1 provides a detailed comparison of key characteristics among human T-bet+ hTregs, GATA3+ hTregs, and RORγt+ hTregs, highlighting their unique profiles, including transcriptional profiles and cytokine production (24, 25).
Cell type CharacteristicT-bet+ hTregsGATA3+ hTregsRORγt+ hTregsKey transcription factorsFoxP3, T-betFoxP3, GATA3FoxP3, RORγtFoxp3 expression (MFI)> 1500> 1000~ 1500CD25 expression (MFI)< 6000< 6000~ 7000PD-1 expression (MFI)~ 2000> 4000< 4000CTLA-4 expression (MFI)~ 500< 1000> 500TIGIT expression (MFI)~ 3000> 4000>3000GARP expression (RNA-seq)Low expressionLow expressionHigh expressionSecreted cytokinesIFN-γ, TNF-αIL-2, IL-4, IL-5, IL-13, IL-21IL-17A, IL-17FUpregulated Th-lineage genesIL7, IL15, TBX21, IRF1, CXCR3, IFNgGATA3, FOSL1, IRF4, IL1A, IL4, IL5, IL9, IL13, IL21, IL24, IL2, CEBPB, IRF8, RUNX3, IL6, NFATC1RORA, RORC, RUNX1, CCR6, IL17A, IL17C, IL7, IL15Upregulated chemokine receptorsCCR2, CCR5, CXR6, CXCR3CXCR5, CXCR4CCR2, CCR5, CXR6, CCR6, CCR9Upregulated chemokineNot AvailableCCL24, CXCL8, CXCL16, CCL3, CCL17CXCL13
Comparison of key characteristics among T-bet+, GATA3+, and RORγt+ hTregs.
The presence of T-bet+ hTregs in the TME and lymph nodes of cancer bearing patients suggests that the TME is not the sole site where these cells can differentiate. Instead, T-bet+ hTregs are likely recruited and retained in the TME, contributing to their high abundance in this environment (14). Tumors can attract and retain CXCR3-expressing cells through the secretion of specific chemokines, primarily C-X-C motif chemokine ligand (CXCL) 9, CXCL10, and CXCL11, which are ligands for the CXCR3 receptor. These chemokines create a gradient that guides CXCR3-expressing immune cells, such as activated CD8+ T cells and natural killer (NK) cells, toward the tumor site (26, 27). Also, CXCR3 plays a crucial role in stabilizing intravascular adhesion of T cells, facilitating their extravasation into the tumor tissue (28). Understanding the mechanisms governing the recruitment and retention of CXCR3-expressing cells including T-bet+ hTregs within the TME is crucial for developing therapeutic strategies aimed at modulating immune cell infiltration to improve antitumor immunity.
2.2 GATA3+ hTregs
GATA3+ hTregs are known to suppress Th2 cell responses (29). The function of Th2 cells in tumor response is complex and multifaceted, with evidence suggesting context-dependent antitumor and pro-tumor effects. Th2 cell were suggested to impair the growth of colon and pancreatic tumors by secreting cytokines, including IL-4, IL-5, and IL-13, which can recruit and activate eosinophils, and other cytotoxic cells into the TME (30, 31). In breast cancer, Th2 cells were shown to induce terminal differentiation of cancer cells, effectively suppressing their malignant potential (32). Of note, Th2 cell responses can also promote tumor growth and metastasis (31). Tregs require IL-4 to differentiate into GATA3+ hTregs (33). GATA3+ hTregs are abundant in melanoma and colorectal cancers. While T-bet+ hTregs and RORγt+ hTregs are prevalent hybrid Tregs in colon, GATA3+ hTregs were found preferentially in tissues compared to the circulation, even in the skin and colon. Although lower expression of Foxp3 is observed in GATA3+ hTregs compared to T-bet+ hTregs and RORγt+ hTregs, these cells are characterized by high levels of IL-2, IL-4, IL-5, and IL-13 cytokines and increased chemotaxis toward CCL17/22 compared to other hybrid Tregs.
GATA3+ hTregs demonstrate superior survival and enhanced proliferative capacity driven by the autocrine IL-2/STAT5 signaling pathway. Additionally, these cells exhibit reduced suppression of Th2-like effector T cells relative to other Treg subsets, likely due to their elevated expression of TIGIT, the only key protein differentially expressed upon activation. Due to enhanced survival, greater migratory potential, and specific suppression of effector T cells, it is suggested that GATA3+ hTregs might promote a tumor-supportive environment (24). GATA3+ hTregs exhibit unique characteristics that may contribute to a tumor-supportive environment, emphasizing the need for further investigation into their role in cancer to uncover potential therapeutic opportunities.
2.3 RORγt+ hTregs
Tregs require IL-6, IL-21, and IL-23 to differentiate into RORγt+ hTregs with capacity to produce IL-17A (33–35). RORγt+ hTregs that secrete IL-17 and express CCR6+ exhibited the highest levels of RORγt, indicating a close resemblance to Th17 cells (36). They are known to suppress Th17 cell responses (37, 38). Th17 cells, particularly through the secretion of IL-17A, can promote tumor angiogenesis (39). Th17 cells contribute to tumor progression as IL-17 triggers IL-6 production, which activates oncogenic signaling pathways, including STAT3. STAT3, in turn, promotes tumor growth by regulating genes involved in angiogenesis (40). It is shown that RORγt+ hTregs are the dominant population in the skin, while the colon is enriched with T-bet+ hTregs and RORγt+ hTregs (24). The equilibrium between Th17 and Tregs is governed by the glycolytic pathway driven by mTOR signaling (41). Overall, there is a lack of comprehensive studies investigating the role of RORγt+ hTregs and their interaction with Th17 cells in tumor immunity. Understanding this dynamic could provide valuable insights into the balance between pro-tumor and antitumor responses with potential clinical applications for targeting these cell populations in cancer therapies.
2.4 T follicular regulatory (Bcl-6+ hTregs) cells
CD4+ T follicular helper (Tfh) cells play a crucial role in supporting B cell functions and are commonly located within tertiary lymphoid structures in tumors. In malignancies derived from Tfh cells or B cells, an elevated frequency of Tfh cells is often linked to poor outcomes. In contrast, in solid organ tumors of non-lymphocytic origin, higher Tfh cell levels are frequently associated with improved prognoses, underscoring their dual and context-dependent roles in cancer (42). In Tfh cells, STAT5 and Bcl-6+ have been reported to bind to shared DNA sequences (43). Bcl-6+ hTregs produce IL-10 and TGF-β, and play a complex and dual roles in tumor immunity (44). Anti-PD-1 and anti-CTLA-4 monotherapy significantly increased the frequency of Bcl-6+ hTregs within tumors (45). Given Bcl-6+ hTregs’ complex and dual role in tumor immunity, further investigation into Bcl-6+ hTregs is crucial to understanding their impact on antibody responses and potential therapeutic strategies in cancer treatment.
3 T-bet+ hTregs in tumor immune regulation
The role of T-bet+ hTregs in cancer is multifaceted and highly context-dependent, exhibiting both pro-tumor and antitumor functions. This duality highlights their remarkable plasticity and ability to adapt to the TME while preserving their regulatory phenotype. It is suggested that T-bet+ hTregs exhibit more rebuts inhibitory capacity in comparison to other hybrid Tregs (18). The inhibitory function of T-bet+ hTregs might rely on different mechanisms, including:
3.1 Cytokine production
Although, T-bet+ hTregs produce cytokines such as IFN-γ typically associated with Th1 cell responses, they also secrete IL-10, and transforming growth factor-beta (TGF-β), produced by conventional Treg cells (Figure 1) (18, 21).
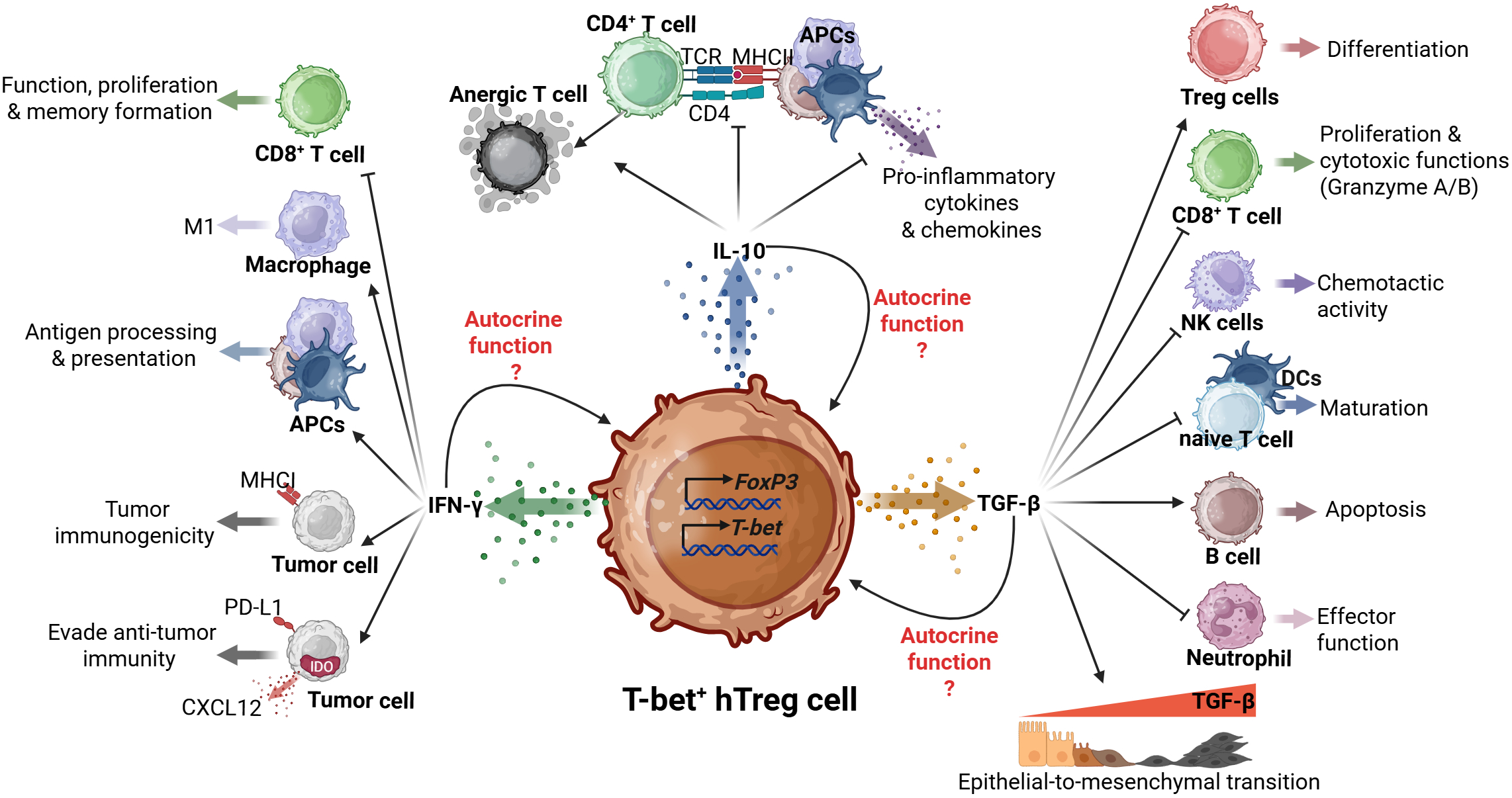
Dual roles of T-bet+ hTregs in tumor progression. The T-bet+ hTregs, characterized by Foxp3 and T-bet expression, exhibits complex interactions through its mainly produced cytokines (IFN-γ, IL-10, and TGF-β). IL-10 production suppresses CD4+ T cell responses and pro-inflammatory cytokine production; potential autocrine function(s) are unclear. TGF-β signaling orchestrates multiple immunomodulatory effects such as Treg differentiation, CD8+ T cell regulation, NK cell chemotaxis, and dendritic cell maturation. These functions demonstrate a potential role of T-bet+ hTregs in coordinating both immunosuppressive and pro-tumoral responses within the TME. Finally, the IFN-γ production influences antigen presentation through APCs, macrophage polarization, and tumor cell responses, including immunogenicity and immune evasion mechanisms.
3.1.1 IL-10
IL-10 is a member of the IL-10 cytokine family with a crucial role in maintaining epithelial tissue integrity, defending against pathogens, and preserving self-tolerance (46). It plays a dual role in cancer immunity exhibiting both antitumor and pro-tumor functions (47). Traditionally, IL-10 was regarded as an immunosuppressive cytokine in the TME. However, recent studies have revealed its antitumor functions. The antitumor or pro-tumor role of IL-10 is linked to the phosphorylation of signal transducer and activator of transcription (STAT) 1 or STAT3. The IL-10 receptor is a heterotetrametric complex consisting of two IL-10Rα and two IL-10Rβ subunits. Upon IL-10 binding, this receptor forms a hexamer, initiating a signaling cascade primarily involving Janus kinase 1 (JAK1) and tyrosine kinase 2 (TYK2), which leads to the phosphorylation of STAT3. Activated STAT3 suppresses excessive immune responses by inhibiting mitogen-activated protein kinase (MAPK), nuclear factor kappa B (NF-κB), and IL-1R production. Conversely, the hexamer can phosphorylate STAT1, enhancing granzyme and IFN-γ production specifically in tumor-resident CD8+ T cells. This effect is not observed in CD8+ T cells isolated from lymph nodes or in CD4+ T cells (48). Therefore, the balance between STAT1 and STAT3 abundance within IL-10R-expressing cells, such as macrophages, dictates the functional outcome of IL-10 signaling. Secretion of IL-10 by T-bet+ hTregs requires a strong TCR activation, STAT4 signaling, and IL-12 signaling (49). IL-4 stimulates IL-10 production in CD4+ T cells, helping to regulate the balance between pro-inflammatory and anti-inflammatory cytokines while encouraging the development of a T-bet+ hTregs phenotype (50). In addition, IL-10 dampens the ability of dendritic cells (DCs) and macrophages to activate antigen-specific CD4+ T cells. In activated macrophages, IL-10 signaling downregulates major histocompatibility complex class (MHC) II and CD86, ultimately disrupting the antigen presentation process to CD4+ T cells by upregulating the E3 ubiquitin ligase, March1 (51, 52). IL-10 also reduces the expression of MHC-I on tumor cells, resulting in tumor immune escape (53). IL-10 plays a pivotal role in modulating both innate and adaptive immune responses by restricting T cell activation and differentiation in lymph nodes, and suppressing pro-inflammatory activity in tissues. This suppression occurs through the reduction of pro-inflammatory cytokines (e.g., IL-1, IL-6, IL-12, IL-18, and TNF-α) and chemokines (e.g., MCP1, MCP5, RANTES, IL-8, IP-10, and MIP-2), potentially leading to impaired pathogen clearance or reduced immunopathology (54). IL-10 can directly inhibit T cell functions by suppressing proliferation, cytokine production (IFN-γ, IL-2) by CD4+ T cells and promoting T cell anergy (54, 55).
3.1.2 Transforming growth factor-beta
TGF-β exhibits a dual role in cancer progression, functioning as a tumor suppressor during the early stages but shifting to promote tumor growth, metastasis, and immune evasion in advanced stages (56–58). TGF-β is produced by a variety of immune and non-immune cells. It is synthesized in an inactive form that requires activation to become functionally active. This activation step serves as a vital regulatory mechanism to control the biological activity of TGF-β (59). Tregs are the primary source of latent TGF-β1 (LTGF-β1) among CD4+ T cells, and uniquely express glycoprotein-A repetitions predominant (GARP) on their surface upon activation. GARP functions as a docking receptor for LTGF-β1, facilitating the release of active TGF-β by integrins (60). TGF-β secreted by Tregs functions in both an autocrine and paracrine manner (61). In normal cells and early-stage cancers, TGF-β acts as a tumor suppressor by inhibiting cell proliferation through repression of c-Myc and induction of cyclin-dependent kinase inhibitors (CDKIs) (62). Within the TME, TGF-β can be secreted by tumor cells, fibroblasts, immune cells, and endothelial cells, and promotes epithelial to mesenchymal transition (EMT) in cancer cells. This process allows advanced-stage tumor cells to migrate from their primary site, enter the bloodstream, colonize distant locations, and form secondary tumors. TGF-β also induces Foxp3 expression, and supports differentiation of naive CD4+ T cells into peripherally-induced Tregs (pTregs), while simultaneously suppressing their conversion to other immune cell types. It inhibits the proliferation and function of cytotoxic CD8+ T cells, reduces the cytotoxicity and chemotactic activity of NK cells, and impairs the maturation of DCs and naïve CD4+ T cells (63, 64). TGF-β also impairs the effector functions of neutrophil and induces apoptosis in B cells. In addition to promoting Foxp3 expression in Tregs, TGF-β inhibits IFN-γ production, and blocks expression of multiple NK cell-related makers, including MHC class I chain-related molecule A (MICA), granzyme A/B, natural killer group 2 member D (NKG2D), natural cytotoxicity receptor 3 (NKP30), and perforin, thereby suppressing immune activity (63). In transformed epithelial cells, TGF-β supports metastasis by upregulating IL-11, parathyroid hormone-related peptide (PTHrP), and matrix metalloprotease (MMP) 9. It also enhances the expression of connective tissue growth factor (CTGF), vascular endothelial growth factor (VEGF), and MMP2, to promote angiogenesis (63). Overall, the pro-tumor effects of TGF-β outweigh its tumor-suppressive functions. Although bulk RNA-seq analysis revealed low GARP expression in T-bet+ hTregs (25), whether GARP in this subset can activate latent TGF-β and modulate T-bet+ hTreg function in an autocrine manner remains to be determined.
3.1.3 IFN-γ
While IFN-γ is widely recognized for its crucial role in stimulating anti-tumor immune responses, it can also have a paradoxical protumor function depending on its concentration and the context within the TME (65). Tregs can acquire Th1-like effector properties while maintaining Foxp3 expression, resulting in IFN-γ+ T-bet+ hTregs. This process is stimulated by IFN-γ, IL-12, or IL-27 and ultimately driven by activation of the PI(3)K-Akt-FOXO signaling pathway (66). Culturing thymic Treg (tTreg) cells with IFN-γ and TGF-β upregulates T-bet and CXCR3 expression. Notably, in the absence of IFN-γ, TGF-β downregulates T-bet expression through a Foxp3-independent mechanism. T-bet also directly enhances the expression of Ifng and IL12rb by binding to their loci. IFN-γ plays a key role in the differentiation of T-bet+ hTregs and is also produced by these cells (20). IFN-γ can activate macrophages and promotes their differentiation into M1 macrophages. IFN-γ also enhances tumor immunogenicity by increasing MHC class I expression on tumor cells, improving antigen presentation, and activating cytotoxic CD8+ T cells to target and eliminate the tumor (67). Deficiency in IFN-γ may cause spontaneous tumor development (60); but in some settings it may function as a pro-tumor molecule. It was reported that IFN-γ can induce programmed cell death ligand 1 (PD-L1), indoleamine 2, 3 dioxygenase (IDO), and CXCL12 in tumor cells supporting their antitumor immune evasion (68–70). Of note, the net pro-tumor or antitumor effects of IFN-γ like that of many other cytokines is determined by a broader network of factors, including the tumor microenvironment (e.g., cytokine milieu, immune cell composition, hypoxia, and metabolic state), tumor type, and the timing and duration of IFN-γ signaling (acute versus chronic exposure) (65, 71, 72). For instance, IFN-γ in melanoma acts through a negative feedback mechanism to constrain anti-tumor immune responses by diminishing the longevity of stem-like T cells (73). During acute and chronic infections, T-bet+ hTregs suppress the function, proliferation, and memory formation of CD8+ T cells (74). A study using a USP15-deficient mouse model revealed that elevated IFN-γ secretion by T cells transforms the TME into an immunosuppressive state, promoting the accumulation of T-bet+ hTregs and CD11b+Gr-1+ myeloid-derived suppressor cells at the tumor site (70). Despite the well-characterized role of IFN-γ in shaping the TME, the mechanistic function of IFN-γ secreted specifically by T-bet+ hTregs remains poorly understood. It is unclear whether the IFN-γ produced by these cells dictates an immunosuppressive TME. Furthermore, the potential autocrine effects of IFN-γ on T-bet+ hTregs is yet to explored. This raises intriguing questions about whether IFN-γ regulates the stability, suppressive function, or metabolic activity of T-bet+ hTregs through self-signaling mechanisms. Further investigation is needed to clarify these pathways and their implications in tumor immunity and therapeutic interventions.
3.2 Expression of immune checkpoint3.2.1 Programmed cell death 1
PD-1 is a immunosuppressive checkpoint expressed by various immune cells, including macrophages, B lymphocytes, DCs, tumor-specific activated T cells, and NK cells under conditions of chronic antigen exposure (75). In addition to activated T cells, tumor infiltrated CD8+ T cells and Tregs also express PD-1, which interacts with its ligands, PD-L1 and PD-L2 (76, 77). It was demonstrated previously that activated T-bet+ hTregs express high levels of PD-1 (14). TCR signaling triggers the activation of various transcription factors, including NFAT2, AP-1, Notch, FOXO1, and TOX, leading to the upregulation of PD-1 (77). PD-1 is critical for the extrathymic differentiation of pTreg cells in the periphery. PD-1-deficient conventional CD4+ T cells show a markedly reduced ability to differentiate into pTregs in various in vivo settings (76). PD-1 signaling also promotes lipid metabolism in tumor-infiltrating Tregs, contributing to their proliferation and suppressive function (Figure 2) (78). Moreover, PD-1 signaling enhances Foxp3 expression in Tregs and strengthens their suppressive characteristics (79). Through PD-1 and PD-L1/PD-L2 signaling with APCs, Tregs maintain immune tolerance in CD4+ and CD8+ T cells. In the TME, Tregs can promote upregulation of PD-1 in tumor-infiltrating antitumor T cells, leading to their exhaustion, and consequently promoting immune evasion tumor cells (80). It was proposed that intermediate levels of PD-1 expression promote T-bet expression during chronic infection, and support the survival of T-bet+ cells. In turn, T-bet maintains PD-1 expression at intermediate levels by repressing Pdcd1 transcription (81). While PD-1 is known to play a significant role in immune regulation, the specific mechanisms by which PD-1 on T-bet+ hTregs may modulate immune responses against tumors remain unclear and warrant further investigation.
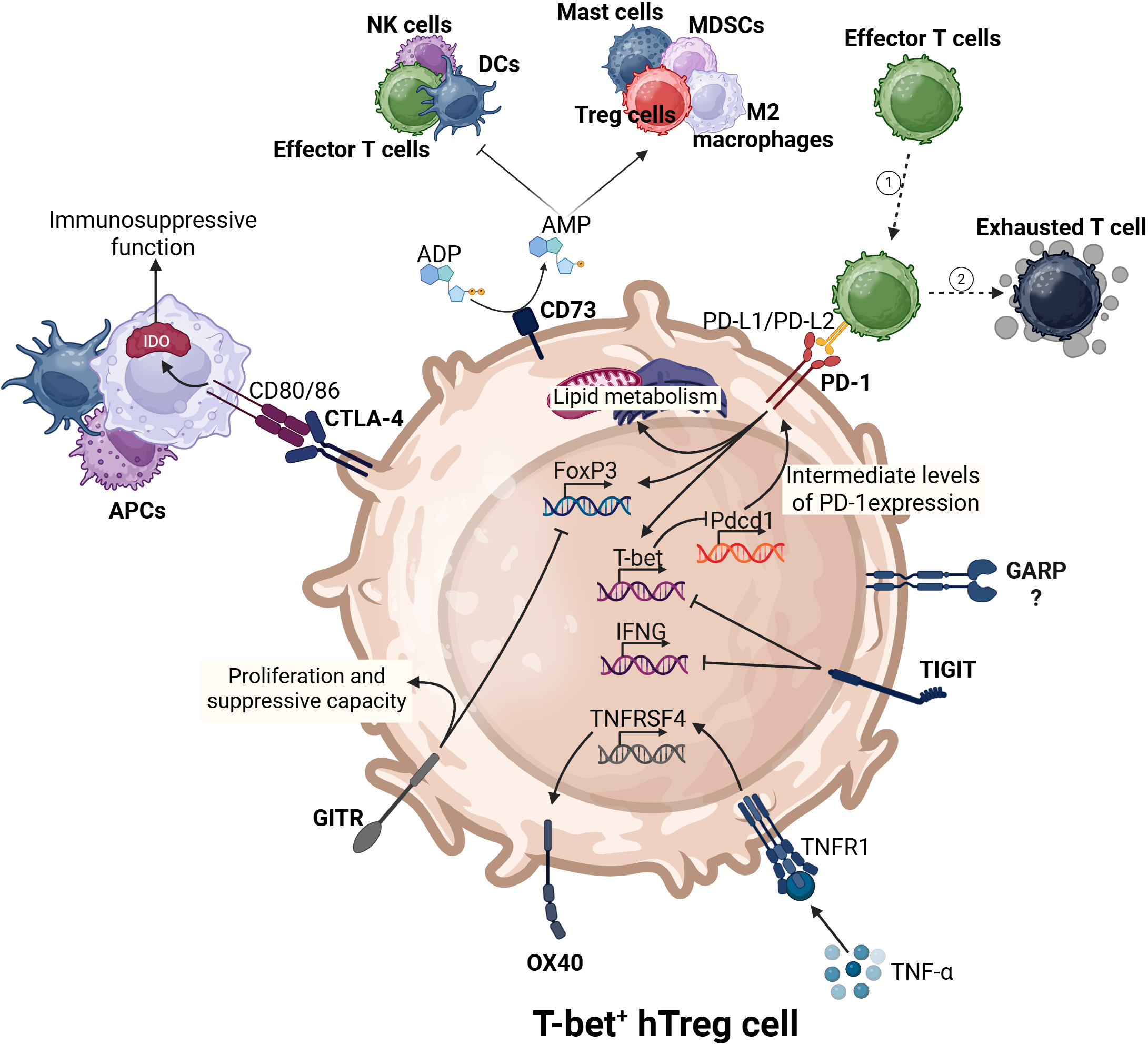
The complex immunoregulatory interactions of T-bet+ hTregs. T-bet+ hTregs express key transcription factors (Foxp3 and T-bet). These cells utilize various immune checkpoints to regulate their activities on the surrounding immune environment. For instance, CD73 promotes pro-tumor immune responses and suppresses antitumor immunity. PD-1 induces the expression of both Foxp3, T-bet, and lipid metabolism. CTLA-4, through the upregulation of IDO in antigen-presenting cells (APCs) can enhance the immunosuppressive nature of the TME.
3.2.2 Cytotoxic T-lymphocyte associated protein 4
CTLA-4 is an inhibitory receptor on T cells and a member of the CD28 family. CD80 and CD86 are known ligands of CTLA-4, and are mostly present on the surface of APCs. Of note, CD80 and CD86 binding to CTLA-4 inhibits T cell activation, while binding to CD28 to activates T cells. Therefore, CTLA-4 and CD28 compete for binding to CD80 or CD86 (82). CTLA-4 is crucial for the suppressive function of Tregs. It interacts with CD80 and CD86 on dendritic cells, transmitting inhibitory signals that downregulate CD80 and CD86 expression and upregulate IDO in dendritic cells, promoting immune tolerance (83, 84). Under normal physiological conditions, IDO maintains immune tolerance; however, in the TME, it acts as an immunosuppressive enzyme (85). Tregs express higher levels of CTLA-4 compared to conventional T cells, and have a greater affinity for binding CD80 and CD86 than CD28. As a result, Tregs outcompete with conventional T cells for CD80 and CD86 binding, leading to reduced activation of conventional T cells (86). Despite reports that T-bet+ hTregs express CTLA-4, the mechanism by which CTLA-4 regulates their suppressive function remains unclear (14).
3.2.3 Glucocorticoid-induced TNFR family related protein
As a member of the TNF receptor family, the GITR immune checkpoint is expressed at low levels on CD8+ and CD4+ T cells but highly expressed on Tregs (87, 88). Its expression levels are frequently associated with proliferation and the immunosuppressive activity of Tregs (89, 90). GITR expression has been reported on T-bet+ hTregs (91). Anti-GITR treatment shifts the immunosuppressive TME of glioblastoma to an immunostimulatory one by specifically targeting glioblastoma Tregs. This treatment converts immunosuppressive Tregs into antitumor Th1-like CD4+ T cells, enhancing the immune response and overcoming resistance to α-PD1 therapy in experimental glioblastoma models (92). The function of GITR in TME is somewhat controversial due to its context-dependent role in T cells. Some studies have reported that triggering GITR signaling with Fc-GITR-L inhibits intratumoral Treg suppressive function but drives CD4+ effector T cell to proliferate (87). Overall, the role of GITR in Tregs, particularly in T-bet+ hTregs remains an area that requires further investigation. Understanding how GITR signaling influences the stability, suppressive function, and interaction of T-bet+ hTregs within the TME could provide valuable insights into their contribution to immune regulation in cancer. Due to the complex nature of Treg cell plasticity, investigating the mechanism behind the function of GITR could help refine therapeutic strategies that target Tregs to enhance antitumor immunity.
3.2.4 Tumor necrosis factor receptor superfamily, member 4
OX40 is a member of the tumor necrosis factor (TNF) receptor/nerve growth factor (NGF) receptor superfamily and a costimulatory molecule expressed on T cells, including Tregs. It plays a complex role in regulating Treg function, typically acting as a negative regulator. Excessive OX40 signaling can impair the suppressive abilities of Tregs and enhance effector T cell responses, potentially disrupting immune tolerance (93, 94). TNF-α signaling elevates OX40 expression and enhances the suppressive capacity of Tregs (19). OX40− T-bet+ hTregs express IFN-γ and exhibit reduced suppressive function, whereas OX40+ T-bet+ hTregs have a suppressive effect on immune responses. OX40+ Tregs are more abundant in cirrhosis and TME, while OX40− Tregs preferentially accumulate in non-cirrhotic chronic HCV liver tissue. OX40 stimulation has been explored as a potential strategy to abolish Treg function and target tumors (19). It was reported that Tregs express higher levels of OX40 in comparison to CD8+ T cells and blockade of OX40 reduced Tregs (95). However, the precise mechanisms underlying the differential effects of OX40 signaling on T-bet+ hTregs remain poorly understood, particularly in terms of their functional plasticity and role in the TME.
3.2.5 T cell immunoreceptor with Ig and ITIM domains
TIGIT is a key inhibitory receptor on Tregs that suppresses pro-inflammatory Th1 and Th17 responses, thereby maintaining immune tolerance (96). The expression of TIGIT has been reported on T-bet+ hTregs (24); however, despite the well-established role of TIGIT in various T cell subsets, its specific function within T-bet+ hTregs remains poorly characterized and is supported by only limited experimental evidence. TIGIT signaling inhibits the production of IFN-γ and the expression of T-bet, while also restoring the suppressive function of Tregs treated with IL-12. Blocking FOXO1 function eliminates the protective effects of TIGIT, suggesting that TIGIT signaling enhances the nuclear localization of FOXO1 (97).
3.2.6 CD73
T-bet+ hTregs express higher levels of CD73 compared to other hybrid Tregs subsets (18). Adenosine triphosphate (ATP) and adenosine diphosphate (ADP) can be released to the extracellular space due to inflammatory conditions such as hypoxia, acute injury, and cancer. Extracellular ATP is dephosphorylated to ADP by CD39, and ADP is further dephosphorylated to adenosine monophosphate (AMP) by CD73 (98). Extracellular AMP triggers intracellular signaling through adenosine receptors such as 1R, A2AR, A2BR, and A3R. These signaling activities result in an anti-inflammatory responses, including boosting accumulation of Tregs, myeloid-derived suppressor cells (MDSCs) and M2 macrophages in tumors (98, 99). CD73 expression has been reported in a wide range of tumors, including ovarian cancer, melanoma, and prostate cancer (98). T-bet+ hTregs might use a similar strategy to suppress antitumor immunity; however, the exact mechanism of CD73 function in these cells remains to be discovered.
3.3 Chemokine receptors3.3.1 C-X-C motif chemokine receptor 3
As a chemokine receptor, CXCR3 plays a crucial role in T cell trafficking and function. CXCR3 is highly expressed on Th1-type CD4+ T cells and effector CD8+ T cells, and its signaling can be triggered by CXCL9, CXCL10, and CXCL11 (100). T-bet upregulates CXCR3 to enhance the migration of Th1 effector cells to inflammatory sites. Similarly, Foxp3+ Tregs can also express T-bet in response to IFN-γ, which drives CXCR3 expression and facilitates the recruitment of these suppressive T cells to inflammatory sites (101). In contrast to Tregs, T-bet+ hTregs express high levels of CXCR3 (14). Within the TME, different cells in response to IFN-γ (e.g. monocytes, endothelial cells, fibroblasts, and cancer cells) secrete CXCL9, CXCL10, and CXCL11 (102). Therefore, paracrine actions of CXCL9, CXCL10, and CXCL11 attract immune cells including Tregs to the TME. CXCR3 also plays an important role in the accumulation and immune suppressive function of tumor-infiltrating Tregs. Treg expression of CXCR3 enables their interaction with type I dendritic cells within the TME to limit the antitumor activities of CD8+ T cells (103). T-bet+ hTregs influence CD8+ T cell activation in the tumor-draining lymph node, although this effect appears to be unrelated to CXCR3 activity (104). CXCR3+ Treg cells demonstrated a greater ability to suppress CD4+CD44+ Th1 effector cells obtained from LCMV-infected mice in vitro (105).
3.3.2 C-C chemokine receptor type 5
CCR5 (CD195) plays an important role during T cell migration by guiding activated T cells to sites of inflammation (106). CCR5 expression is markedly higher on Th1-like Tregs, making it a reliable marker for identifying T-bet+ hTregs (91). T-bet+ hTregs in the peripheral blood of untreated, relapsing-remitting MS (RRMS) patients exhibit higher levels of T-bet, CXCR3, CCR5, and IFN-γ, along with reduced levels of TGF-β and CTLA-4 (19). CCR5 expression on T-bet+ hTregs allows their migration to inflammatory sites where CCL5, the ligand for CCR5 is produced, and potentially facilitates their immune suppressive function (107).
3.4 Self-regulation and plasticity
Cell fate is determined by the interplay between extrinsic environmental signals and intrinsic, cell-autonomous programs. The relative influence of these factors varies by cell type and developmental stage (108). Self-regulation: While Th1 responses clear pathogens, it can also damage healthy host tissues (109). CD4+ T cells including Th1 cells can utilize IL-10 as a self-regulatory mechanism during pathogen clearance to reduce immunopathology (110). During Leishmania major, Toxoplasma gondii infection and excessive inflammation, IL-10 production by Th1 cells is suggested to function as a self-regulatory mechanism that helps limit tissue damage (109, 111). Indeed, therapeutically inducing the switch from IFN-γ+ to IL-10+ Th1 cells is a promising approach; however, this depends on identifying the molecular checkpoints that govern Th1 development and evaluating their therapeutic potential (112). Tregs also possess an intrinsic self-regulatory system. Foxp3, in particular, interacts with multiple cofactors to create complex positive and negative feedback loops that precisely control Treg development, stability, and suppressive function (113). For instance, the positive feedback loop is reinforced by IL-2, which binds to the high-affinity IL-2 receptor on most Treg cells, preventing apoptosis through upregulation of MCL1 expression (114). Plasticity: While IL-4 treatment induces Th1 cells to upregulate GATA-3 and adopt a hybrid T-bet+GATA-3+ Th1/Th2 phenotype, high T-bet expression remains essential for maintaining Th1 phenotypic stability (115). In tumors, IFN-γ producing Th1 cells can differentiate into Treg cells under the influence of TGF-β signaling (116). Plasticity in Tregs is controlled by both metabolic and transcriptional mechanisms. T-bet+ hTregs differentiate via IL-12–driven activation of the PI3K/Akt/Foxo pathway, with HIF-1α promoting glycolysis and directly binding the Ifng gene to enhance IFN-γ expression (117). T-bet+ hTregs can arise from Th1 cells or conventional Tregs through cellular plasticity (116, 118, 119). However, the extent to which self-regulation and plasticity contribute to their development from each source remains unclear. Overall, understanding the balance between self-regulation and plasticity during differentiation of T-bet+ hTregs is essential to unveiling how they establish and maintain their identity.
4 T-bet+ hTregs as a new candidate to fight cancer
Tregs play a crucial role in maintaining immune homeostasis by suppressing excessive immune responses. Nevertheless, within the TME Tregs can inhibit antitumor immunity, promoting tumor progression. In cancer patients, increased infiltration of Tregs within tumor tissues is often associated with poor clinical outcomes (120). As a result, targeting Tregs has become a key focus in cancer immunotherapy. Depletion of Tregs has been shown to significantly boost antitumor immunity; however, systemic depletion of Tregs can lead to severe autoimmune diseases (7). Different immunotherapies have been examined to target Tregs, including anti-CTLA-4 agents such as ipilimumab and tremelimumab, but their effectiveness in depleting intratumoral Tregs in humans has been limited. It was previously shown that while these agents increase infiltration of CD4+ and CD8+ T cells within tumors, they do not significantly reduce the number of Foxp3+ Tregs in the tumor microenvironment (121). Immune checkpoint blockade therapy often produces longer-lasting responses compared to chemotherapy or targeted treatments (122, 123). Yet, as global clinical data continues to grow, its limitations and adverse effects are becoming evident. A significant challenge with immune checkpoint blockade therapy is its low efficacy in many cancers, with response rates typically ranging from 10% to 30%. Moreover, for some major cancer types, such as microsatellite-stable colorectal cancer, anti-PD-1/PD-L1 therapy demonstrates minimal effectiveness (124). In addition to immune checkpoint blockade therapies, other strategies have been employed to target Tregs in cancer, including antibody-drug-conjugates (ADC), small-interfering RNA (siRNA), and peptide-based approaches. Various clinical trials and preclinical studies have used these strategies to target molecules such as CD25, CCR4, CTLA-4, STAT3, PD-1, Foxp3, and 4-1BB (CD137) in the TME. More specifically, peptide targeting has been used to target Foxp3, β-catenin, TGF-β1, NRP-1, and CXCR4 in Tregs within tumors. Although knowledge about these strategies is growing, their side effects remain largely unknown (125). Therefore, more effective therapies are still required to combat cancer. A promising strategy involves appreciating the heterogeneity of Tregs within the TME and investigating the roles of specific Tregs subsets. This approach could open new opportunities for developing treatments that selectively target these subsets in cancer patients.
Tregs within tumors exhibited elevated expression of T-bet, which was crucial for their activity in the TME. Furthermore, CD39 was prominently expressed on T-bet+ Tregs in both mouse and human tumors and played a key role in enabling these cells to suppress CD8+ T cell responses (116). For instance, the presence of T-bet+ hTregs has been reported in various human cancers, including ovarian cancer, lung cancer, colorectal cancer, hepatocellular carcinoma, and oral squamous cell carcinoma (20). This Treg subset is stable even under inflammatory or otherwise unfavorable conditions (126). T-bet+ hTregs represent a specific subset of Tregs characterized by the expression of CXCR3. Therefore, combining immunotherapies such as anti-CTLA-4 and anti-PD-1 with CXCR3 blockade could offer a novel approach to targeting T-bet+ hTregs. Several CXCR3 blockers have been reported in preclinical studies for various diseases, including autoimmune, inflammatory diseases, and transplant rejection (127). Preclinical studies using AMG487, CXCR3 blocker, demonstrated significant reductions in metastasis in murine models of breast cancer and osteosarcoma (128, 129). AMG487 has also been evaluated in clinical trials for the treatment of psoriasis and rheumatoid arthritis (130). In another clinical trial, ACT-777991 was evaluated for safety, tolerability, and pharmacokinetics in single- and multiple-ascending doses in healthy subjects. However, neither AMG487 nor ACT-777991 has yet been assessed in clinical trials for cancer (131). Inhibition of CXCR3 on T-bet+ hTregs could hinder their migration to tumor sites, potentially reducing their ability to suppress local immune responses. However, targeting CXCR3 may also impair the migration of antitumor immune cells to the tumor site. By selectively inhibiting the recruitment of T-bet+ hTregs to the TME, it may be possible to enhance the effectiveness of existing therapies and improve clinical outcomes. Furthermore, targeting this subset could help mitigate the off-target effects seen with broader Treg depletion strategies, minimizing the risk of autoimmune complications. Thus, refining our understanding of Treg subtypes and their specific roles in cancer immunity is crucial for advancing therapeutic strategies aimed at overcoming the challenges associated with current cancer immunotherapies.
5 Discussion and future perspectives
In conclusion, the discovery of T-bet+ hTregs has added a new layer of complexity to our understanding of tumor immunology and the potential for cancer immunotherapy. These cells, characterized by the co-expression of Foxp3 and T-bet, along with the production of IFN-γ, represent a unique subset of Tregs with high plasticity and context-dependent functions within the TME. T-bet+ hTregs exhibit both pro-tumor and antitumor properties, highlighting their adaptability to the TME. They suppress antitumor immunity through various mechanisms, including cytokine production (IL-10, TGF-β, IFN-γ, and TNF-α) and expression of immune checkpoint molecules (PD-1, CTLA-4, GITR, OX40, and TIGIT). Their high expression of chemokine receptors, particularly CXCR3 and CCR5, facilitates their migration to inflammatory sites and tumors, potentially enhancing their immunosuppressive functions. The heterogeneity of Tregs within the TME, including the T-bet+ hTregs subset, presents both challenges and opportunities for cancer immunotherapy. While global Treg depletion has shown promise in boosting antitumor immunity, it carries the risk of severe autoimmune complications. Targeting specific Tregs subsets, such as T-bet+ hTregs could offer a more nuanced approach to cancer treatment. However, strategies to selectively target specific cell types remain limited. For example, the emerging PROTAC (Proteolysis-Targeting Chimera) platform can efficiently degrade a defined protein within a cell, yet achieving selective degradation of a specific protein in a particular cell type introduces additional layers of complexity and challenges in feasibility. If such a system were available, selectively targeting both FOXP3 and T-bet, rather than each factor individually, in T-bet+ hTreg cells could more effectively diminish their capacity to suppress antitumor immunity. Currently, feasible strategies for targeting T-bet+ hTregs include combining existing immunotherapies (e.g., anti-CTLA-4 and anti-PD-1) with CXCR3 blockade or developing drugs that specifically inhibit CXCR3 expression on these cells. Such approaches could prevent their migration to tumor sites and reduce their immunosuppressive effects, potentially enhancing the efficacy of current therapies while minimizing off-target effects. In addition, emerging technologies, including spatial transcriptomics, hTreg-specific gene editing models, and single-cell multi-omics approaches (such as scRNA-seq and CITE-seq), now enable precise dissection of T-bet+ hTreg heterogeneity, localization, and function within the TME. These tools provide unprecedented insight into their suppressive mechanisms and interactions with other immune cells. Together, they pave the way for developing targeted strategies to modulate Treg subsets while minimizing off-target effects. It is worth noting that only limited information is currently available regarding the specific roles of T-bet+ hTregs in cancer and their potential as therapeutic targets. More research is needed to fill these knowledge gaps and inform the development of more effective cancer immunotherapies.
StatementsAuthor contributions
PA-S: Investigation, Conceptualization, Writing – original draft, Visualization. MS-A: Conceptualization, Investigation, Writing – original draft, Visualization. JK: Writing – review & editing. EA-A: Writing – review & editing, Resources, Conceptualization, Funding acquisition, Supervision.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study was supported by the Pelotonia Institute for Immuno-Oncology (PIIO) and start-up funding support to EA-A. The content is solely the responsibility of the authors and does not necessarily represent the official views of the PIIO.
Acknowledgments
We acknowledge resources from the PIIO and Immune Monitoring and Discovery Platform at the OSU Comprehensive Cancer Center (P30CA016058). Figures were created with BioRender.com.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
AndersonNMSimonMC. The tumor microenvironment. Curr biology: CB. (2020) 30:R921–r5. doi: 10.1016/j.cub.2020.06.081
DixonKOTabakaMSchrammMAXiaoSTangRDionneDet al. TIM-3 restrains anti-tumour immunity by regulating inflammasome activation. Nature. (2021) 595:101–6. doi: 10.1038/s41586-021-03626-9
GeRWangZChengL. Tumor microenvironment heterogeneity an important mediator of prostate cancer progression and therapeutic resistance. NPJ Precis Oncol. (2022) 6:31. doi: 10.1038/s41698-022-00272-w
MayerSMiloTIsaacsonAHalperinCMiyaraSSteinYet al. The tumor microenvironment shows a hierarchy of cell-cell interactions dominated by fibroblasts. Nat Commun. (2023) 14:5810. doi: 10.1038/s41467-023-41518-w
FengLQianHYuXLiuKXiaoTZhangCet al. Heterogeneity of tumor-infiltrating lymphocytes ascribed to local immune status rather than neoantigens by multi-omics analysis of glioblastoma multiforme. Sci Rep. (2017) 7:6968. doi: 10.1038/s41598-017-05538-z
ZhangJHuangYHanYDongDCaoYChenXet al. Immune microenvironment heterogeneity of concurrent adenocarcinoma and squamous cell carcinoma in multiple primary lung cancers. NPJ Precis Oncol. (2024) 8:55. doi: 10.1038/s41698-024-00548-3
TanakaASakaguchiS. Regulatory T cells in cancer immunotherapy. Cell Res. (2017) 27:109–18. doi: 10.1038/cr.2016.151
RosenblumMDWaySSAbbasAK. Regulatory T cell memory. Nat Rev Immunol. (2016) 16:90–101. doi: 10.1038/nri.2015.1
KimM-CBorcherdingNAhmedKKVoigtAPVishwakarmaAKolbRet al. CD177 modulates the function and homeostasis of tumor-infiltrating regulatory T cells. Nat Commun. (2021) 12:5764. doi: 10.1038/s41467-021-26091-4
KitzASingerEHaflerD. Regulatory T cells: from discovery to autoimmunity. Cold Spring Harbor Perspect Med. (2018) 8. doi: 10.1101/cshperspect.a029041
KachlerKHolzingerCTrufaDISirbuHFinottoS. The role of Foxp3 and Tbet co-expressing Treg cells in lung carcinoma. Oncoimmunology. (2018) 7:e1456612. doi: 10.1080/2162402X.2018.1456612
SantegoetsSJDuurlandCLJordanovaESvan HamJJEhsanIvan EgmondSLet al. Tbet-positive regulatory T cells accumulate in oropharyngeal cancers with ongoing tumor-specific type 1 T cell responses. J immunotherapy cancer. (2019) 7:14. doi: 10.1186/s40425-019-0497-0
OkamotoMSasaiMKurataniAOkuzakiDAraiMWingJBet al. A genetic method specifically delineates Th1-type Treg cells and their roles in tumor immunity. Cell Rep. (2023) 42:112813. doi: 10.1016/j.celrep.2023.112813
RamirezDETurkMJ. Th1-like Treg cells are dressed to suppress anti-tumor immunity. Immunity. (2023) 56:1437–9. doi: 10.1016/j.immuni.2023.06.014
PiconeseSWalkerLSKDominguez-VillarM. Editorial: control of regulatory T cell stability, plasticity, and function in health and disease. Front Immunol. (2020) 11:611591. doi: 10.3389/fimmu.2020.611591
SawantDVVignaliDA. Once a treg, always a treg? Immunol Rev. (2014) 259:173–91.
TanoueTAtarashiKHondaK. Development and maintenance of intestinal regulatory T cells. Nat Rev Immunol. (2016) 16:295–309. doi: 10.1038/nri.2016.36
ZhangRMiaoJZhangKZhangBLuoXSunHet al. Th1-like treg cells are increased but deficient in function in rheumatoid arthritis. Front Immunol. (2022) 13:863753. doi: 10.3389/fimmu.2022.863753
KitzADominguez-VillarM. Molecular mechanisms underlying Th1-like Treg generation and function. Cell Mol Life sciences: CMLS. (2017) 74:4059–75. doi: 10.1007/s00018-017-2569-y
Contreras-CastilloEGarcía-RasillaVYGarcía-PatiñoMGLicona-LimónP. Stability and plasticity of regulatory T cells in health and disease. J Leukocyte Biol. (2024) 116:33–53. doi: 10.1093/jleuko/qiae049
DuhenTDuhenRLanzavecchiaASallustoFCampbellDJ. Functionally distinct subsets of human FOXP3+ Treg cells that phenotypically mirror effector Th cells. Blood. (2012) 119:4430–40. doi: 10.1182/blood-2011-11-392324
LeeGR. IRF8: identity-keeper for suppressive Th1-like Treg cells. Cell Mol Immunol. (2018) 15:1080–1. doi: 10.1038/s41423-018-0044-9
KleinewietfeldMHaflerDA. The plasticity of human Treg and Th17 cells and its role in autoimmunity. Semin Immunol. (2013) 25:305–12. doi: 10.1016/j.smim.2013.10.009
HalimLRomanoMMcGregorRCorreaIPavlidisPGragedaNet al. An atlas of human regulatory T helper-like cells reveals features of th2-like tregs that support a tumorigenic environment. Cell Rep. (2017) 20:757–70. doi: 10.1016/j.celrep.2017.06.079
HöllbacherBDuhenTMotleySKlicznikMMGratzIKCampbellDJ. Transcriptomic profiling of human effector and regulatory T cell subsets identifies predictive population signatures. ImmunoHorizons. (2020) 4:585–96. doi: 10.4049/immunohorizons.2000037
KohliKPillarisettyVGKimTS. Key chemokines direct migration of immune cells in solid tumors. Cancer Gene Ther. (2022) 29:10–21. doi: 10.1038/s41417-021-00303-x
ReyndersNAbboudDBaragliANomanMZRogisterBNiclouSPet al. The distinct roles of CXCR3 variants and their ligands in the tumor microenvironment. Cells. (2019) 8. doi: 10.3390/cells8060613
MikuckiMEFisherDTMatsuzakiJSkitzkiJJGaulinNBMuhitchJBet al. Non-redundant requirement for CXCR3 signalling during tumoricidal T-cell trafficking across tumour vascular checkpoints. Nat Commun. (2015) 6:7458. doi: 10.1038/ncomms8458
ZhengYChaudhryAKasAdeRoosPKimJMChuT-Tet al. Regulatory T-cell suppressor program co-opts transcription factor IRF4 to control TH2 responses. Nature. (2009) 458:351–6. doi: 10.1038/nature07674
JacenikDKaragiannidisIBeswickEJ. Th2 cells inhibit growth of colon and pancreas cancers by promoting anti-tumorigenic responses from macrophages and eosinophils. Br J Cancer. (2023) 128:387–97. doi: 10.1038/s41416-022-02056-2
SchreiberSHammersCMKaaschAJSchravenBDudeckAKahlfussS. Metabolic interdependency of th2 cell-mediated type 2 immunity and the tumor microenvironment. Front Immunol. (2021) 12:632581. doi: 10.3389/fimmu.2021.632581
BoieriMMalishkevichAGuennounRMarcheseEKroonSTrericeKEet al. CD4+ T helper 2 cells suppress breast cancer by inducing terminal differentiation. J Exp Med. (2022) 219:e20201963. doi: 10.1084/jem.20201963
BarnesMJPowrieF. Hybrid Treg cells: steel frames and plastic exteriors. Nat Immunol. (2009) 10:563–4. doi: 10.1038/ni0609-563
JungMKKwakJ-EShinE-C. IL-17A-producing foxp3+ Regulatory T cells and human diseases. Immune Netw. (2017) 17:276–86. doi: 10.4110/in.2017.17.5.276
OmenettiSPizarroTT. The treg/th17 axis: A dynamic balance regulated by the gut microbiome. (2015) 6:. doi: 10.3389/fimmu.2015.00639
FuruyamaKKondoYKanekoSShimizuMTanimuraRTsuboiHet al. Effecter Th17-like regulatory T cells associate with the pathogenesis of rheumatoid arthritis. Rheumatol (Oxford England). (2022) 62:e4–6. doi: 10.1093/rheumatology/keac382
ChaudhryARudraDTreutingPSamsteinRMLiangYKasAet al. CD4+ Regulatory T cells control TH17 responses in a stat3-dependent manner. Sci (New York NY). (2009) 326:986–91. doi: 10.1126/science.1172702
ThomasRQiaoSYangX. Th17/treg imbalance: implications in lung inflammatory diseases. Int J Mol Sci. (2023) 24. doi: 10.3390/ijms24054865
BaileySRNelsonMHHimesRALiZMehrotraSPaulosCM. Th17 cells in cancer: the ultimate identity crisis. (2014) 5:. doi: 10.3389/fimmu.2014.00276
YuHKortylewskiMPardollD. Crosstalk between cancer and immune cells: role of STAT3 in the tumour microenvironment. Nat Rev Immunol. (2007) 7:41–51. doi: 10.1038/nri1995
QinYGaoCLuoJ. Metabolism characteristics of th17 and regulatory T cells in autoimmune diseases. (2022) 13:. doi: 10.3389/fimmu.2022.828191
Gutiérrez-MeloNBaumjohannD. T follicular helper cells in cancer. Trends Cancer. (2023) 9:309–25. doi: 10.1016/j.trecan.2022.12.007
LiuXLuHChenTNallaparajuKCYanXTanakaSet al. Genome-wide analysis identifies bcl6-controlled regulatory networks during T follicular helper cell differentiation. Cell Rep. (2016) 14:1735–47. doi: 10.1016/j.celrep.2016.01.038
HaoHNakayamadaSYamagataKOhkuboNIwataSInoueYet al. Conversion of T follicular helper cells to T follicular regulatory cells by interleukin-2 through transcriptional regulation in systemic lupus erythematosus. Arthritis Rheumatol (Hoboken NJ). (2021) 73:132–42. doi: 10.1002/art.41457
EschweilerSClarkeJRamírez-SuásteguiCPanwarBMadrigalACheeSJet al. Intratumoral follicular regulatory T cells curtail anti-PD-1 treatment efficacy. Nat Immunol. (2021) 22:1052–63. doi: 10.1038/s41590-021-00958-6
NiGZhangLYangXLiHMaBWaltonSet al. Targeting interleukin-10 signalling for cancer immunotherapy, a promising and complicated task. Hum Vaccines immunotherapeutics. (2020) 16:2328–32. doi: 10.1080/21645515.2020.1717185
ManninoMHZhuZXiaoHBaiQWakefieldMRFangY. The paradoxical role of IL-10 in immunity and cancer. Cancer Letters. (2015) 367:103–7. doi: 10.1016/j.canlet.2015.07.009
SalkeniMANaingA. Interleukin-10 in cancer immunotherapy: from bench to bedside. Trends Cancer. (2023) 9:716–25. doi: 10.1016/j.trecan.2023.05.003
CarliniVNoonanDMAbdalalemEGolettiDSansoneCCalabroneLet al. The multifaceted nature of IL-10: regulation, role in immunological homeostasis and its relevance to cancer, COVID-19 and post-COVID conditions. (2023) 14:. doi: 10.3389/fimmu.2023.1161067
MitchellREHassanMBurtonBRBrittonGHillEVVerhagenJet al. IL-4 enhances IL-10 production in Th1 cells: implications for Th1 and Th2 regulation. Sci Rep. (2017) 7:11315. doi: 10.1038/s41598-017-11803-y
MittalSKChoKJIshidoSRochePA. Interleukin 10 (IL-10)-mediated immunosuppression: MARCH-I INDUCTION REGULATES ANTIGEN PRESENTATION BY MACROPHAGES BUT NOT DENDRITIC CELLS. J Biol Chem. (2015) 290:27158–67. doi: 10.1074/jbc.M115.682708
SaraivaMO’GarraA. The regulation of IL-10 production by immune cells. Nat Rev Immunol. (2010) 10:170–81. doi: 10.1038/nri2711
RallisKSCorriganAEDadahHGeorgeAMKeshwaraSMSiderisMet al. Cytokine-based cancer immunotherapy: challenges and opportunities for IL-10. Anticancer Res. (2021) 41:3247. doi: 10.21873/anticanres.15110
CouperKNBlountDGRileyEM. IL-10: the master regulator of immunity to infection. J Immunol. (2008) 180:5771–7. doi: 10.4049/jimmunol.180.9.5771
SullivanKMJiangXGuhaPLaustedCCarterJAHsuCet al. Blockade of interleukin 10 potentiates antitumour immune function in human colorectal cancer liver metastases. Gut. (2023) 72:325. doi: 10.1136/gutjnl-2021-325808
KimB-GMalekEChoiSHIgnatz-HooverJJDriscollJJ. Novel therapies emerging in oncology to target the TGF-β pathway. J Hematol Oncol. (2021) 14:55. doi: 10.1186/s13045-021-01053-x
ShiXYangJDengSXuHWuDZengQet al. TGF-β signaling in the tumor metabolic microenvironment and targeted therapies. J Hematol Oncol. (2022) 15:135. doi: 10.1186/s13045-022-01349-6
PrincipeDRDollJABauerJJungBMunshiHGBartholinLet al. TGF-β: duality of function between tumor prevention and carcinogenesis. J Natl Cancer Institute. (2014) 106:djt369. doi: 10.1093/jnci/djt369
TravisMASheppardD. TGF-β activation and function in immunity. Annu Rev Immunol. (2014) 32:51–82. doi: 10.1146/annurev-immunol-032713-120257
MoreauJMVelegrakiMBolyardCRosenblumMDLiZ. Transforming growth factor-β1 in regulatory T cell biology. Sci Immunol. (2022) 7:eabi4613. doi: 10.1126/sciimmunol.abi4613
BrownHEsterházyD. Paying a price twice: dose-dependent effects of treg cell-derived TGF- β on tolerance. Immunity. (2020) 53:1128–30. doi: 10.1016/j.immuni.2020.11.008
LiuSChenSZengJ. TGF−β signaling: A complex role in tumorigenesis (Review). Mol Med Rep. (2018) 17:699–704.
LiuSRenJten DijkeP. Targeting TGFβ signal transduction for cancer therapy. Signal Transduction Targeted Ther. (2021) 6:8. doi: 10.1038/s41392-020-00436-9
LazarovaMSteinleA. Impairment of NKG2D-mediated tumor immunity by TGF-β. (2019) 10:. doi: 10.3389/fimmu.2019.02689
LiuX. The paradoxical role of IFN-γ in cancer: Balancing immune activation and immune evasion. Pathol – Res Practice. (2025) 272:156046. doi: 10.1016/j.prp.2025.156046
ChoiGNaHKuenDSKimBSChungY. Autocrine TGF-β1 maintains the stability of foxp3(+) regulatory T cells via IL-12Rβ2 downregulation. Biomolecules. (2020) 10. doi: 10.3390/biom10060819
ZaidiMRMerlinoG. The two faces of interferon-γ in cancer. Clin Cancer Res. (2011) 17:6118–24. doi: 10.1158/1078-0432.CCR-11-0482
SharmaPHu-LieskovanSWargoJARibasA. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell. (2017) 168:707–23. doi: 10.1016/j.cell.2017.01.017
AlspachELussierDMSchreiberRD. Interferon γ and its important roles in promoting and inhibiting spontaneous and therapeutic cancer immunity. Cold Spring Harbor Perspect Biol. (2019) 11. doi: 10.1101/cshperspect.a028480
ZouQJinJXiaoYZhouXHuHChengXet al. T cell intrinsic USP15 deficiency promotes excessive IFN-γ Production and an immunosuppressive tumor microenvironment in MCA-induced fibrosarcoma. Cell Rep. (2015) 13:2470–9. doi: 10.1016/j.celrep.2015.11.046
MojicMTakedaKHayakawaY. The dark side of IFN-γ: its role in promoting cancer immunoevasion. Int J Mol Sci. (2018) 19.
CastroFCardosoAPGonçalvesRMSerreKOliveiraMJ. Interferon-gamma at the crossroads of tumor immune surveillance or evasion. (2018) 9:. doi: 10.3389/fimmu.2018.00847
MazetJMMahaleJNTongOWatsonRALechuga-ViecoAVPirgovaGet al. IFNγ signaling in cytotoxic T cells restricts anti-tumor responses by inhibiting the maintenance and diversity of intra-tumoral stem-like T cells. Nat Commun. (2023) 14:321. doi: 10.1038/s41467-023-35948-9
Gocher-DemskeAMCuiJSzymczak-WorkmanALVignaliKMLatiniJNPiekloGPet al. IFNγ-induction of TH1-like regulatory T cells controls antiviral responses. Nat Immunol. (2023) 24:841–54. doi: 10.1038/s41590-023-01453-w
TangQChenYLiXLongSShiYYuYet al. The role of PD-1/PD-L1 and application of immune-checkpoint inhibitors in human cancers. Front Immunol. (2022) 13:964442. doi: 10.3389/fimmu.2022.964442
ChenXFoscoDKlineDEMengLNishiSSavagePAet al. PD-1 regulates extrathymic regulatory T-cell differentiation. Eur J Immunol. (2014) 44:2603–16. doi: 10.1002/eji.201344423
KimMJHaSJ. Differential role of PD-1 expressed by various immune and tumor cells in the tumor immune microenvironment: expression, function, therapeutic efficacy, and resistance to cancer immunotherapy. Front Cell Dev Biol. (2021) 9:767466. doi: 10.3389/fcell.2021.767466
KimMJKimKParkHJKimG-RHongKHOhJHet al. Deletion of PD-1 destabilizes the lineage identity and metabolic fitness of tumor-infiltrating regulatory T cells. Nat Immunol. (2023) 24:148–61. doi: 10.1038/s41590-022-01373-1
CaiJWangDZhangGGuoX. The role of PD-1/PD-L1 axis in treg development and function: implications for cancer immunotherapy. OncoTargets Ther. (2019) 12:8437–45. doi: 10.2147/OTT.S221340
GianchecchiEFierabracciA. Inhibitory receptors and pathways of lymphocytes: the role of PD-1 in treg development and their involvement in autoimmunity onset and cancer progression. Front Immunol. (2018) 9:2374. doi: 10.3389/fimmu.2018.02374
OdorizziPMPaukenKEPaleyMASharpeAWherryEJ. Genetic absence of PD-1 promotes accumulation of terminally differentiated exhausted CD8+ T cells. J Exp Med. (2015) 212:1125–37. doi: 10.1084/jem.20142237
Van CoillieSWiernickiBXuJ. Molecular and cellular functions of CTLA-4. Adv Exp Med Biol. (2020) 1248:7–32.
MellorALMunnDH. Ido expression by dendritic cells: tolerance and tryptophan catabolism. Nat Rev Immunol. (2004) 4:762–74. doi: 10.1038/nri1457
WalkerLSK. EFIS Lecture: Understanding the CTLA-4 checkpoint in the maintenance of immune homeostasis. Immunol Letters. (2017) 184:43–50. doi: 10.1016/j.imlet.2017.02.007
MunnDHMellorAL. Indoleamine 2,3-dioxygenase and tumor-induced tolerance. J Clin Invest. (2007) 117:1147–54. doi: 10.1172/JCI31178
RowshanravanBHallidayNSansomDM. CTLA-4: a moving target in immunotherapy. Blood. (2018) 131:58–67. doi: 10.1182/blood-2017-06-741033
EphremAEpsteinALStephensGLThorntonAMGlassDShevachEM. Modulation of Treg cells/T effector function by GITR signaling is context-dependent. Eur J Immunol. (2013) 43:2421–9. doi: 10.1002/eji.201343451
FacciabeneAMotzGTCoukosG. T-regulatory cells: key players in tumor immune escape and angiogenesis. Cancer Res. (2012) 72:2162–71. doi: 10.1158/0008-5472.CAN-11-3687
TianJZhangBRuiKWangS. The role of GITR/GITRL interaction in autoimmune diseases. (2020) 11:. doi: 10.3389/fimmu.2020.588682
LiaoGNayakSRegueiroJRBergerSBDetreCRomeroXet al. GITR engagement preferentially enhances proliferation of functionally competent CD4+CD25+FoxP3+ regulatory T cells. Int Immunol. (2010) 22:259–70. doi: 10.1093/intimm/dxq001
ButcherMJFilipowiczARWaseemTCMcGaryCMCrowKJMagilnickNet al. Atherosclerosis-driven treg plasticity results in formation of a dysfunctional subset of plastic IFNγ+ Th1/tregs. Circ Res. (2016) 119:1190–203. doi: 10.1161/CIRCRESAHA.116.309764
AmoozgarZKloepperJRenJTayREKazerSWKinerEet al. Targeting Treg cells with GITR activation alleviates resistance to immunotherapy in murine glioblastomas. Nat Commun. (2021) 12:2582. doi: 10.1038/s41467-021-22885-8
RubyCEYatesMAHirschhorn-CymermanDChlebeckPWolchokJDHoughtonANet al. Cutting edge: OX40 agonists can drive regulatory T cell expansion if the cytokine milieu is right. J Immunol. (2009) 183:4853–7. doi: 10.4049/jimmunol.0901112
Kupiec-WeglinskiJW. OX40 costimulation and regulatory T cells. Blood. (2007) 110:2217–8. doi: 10.1182/blood-2007-07-097642
FuYLinQZhangZZhangL. Therapeutic strategies for the costimulatory molecule OX40 in T-cell-mediated immunity. Acta Pharm Sin B. (2020) 10:414–33. doi: 10.1016/j.apsb.2019.08.010
JollerNLozanoEBurkettPRPatelBXiaoSZhuCet al. Treg cells expressing the coinhibitory molecule TIGIT selectively inhibit proinflammatory Th1 and Th17 cell responses. Immunity. (2014) 40:569–81. doi: 10.1016/j.immuni.2014.02.012
LuccaLEAxisaPPSingerERNolanNMDominguez-VillarMHaflerDA. TIGIT signaling restores suppressor function of Th1 Tregs. JCI Insight. (2019) 4. doi: 10.1172/jci.insight.124427
ChiarellaAMRyuYKManjiGARustgiAK. Extracellular ATP and adenosine in cancer pathogenesis and treatment. Trends Cancer. (2021) 7:731–50. doi: 10.1016/j.trecan.2021.04.008
HarveyJBPhanLHVillarrealOEBowserJL. CD73’s potential as an immunotherapy target in gastrointestinal cancers. (2020) 11:. doi: 10.3389/fimmu.2020.00508
GroomJRLusterAD. CXCR3 in T cell function. Exp Cell Res. (2011) 317:620–31. doi: 10.1016/j.yexcr.2010.12.017
KuoPTZengZSalimNMattarolloSWellsJWLeggattGR. The role of CXCR3 and its chemokine ligands in skin disease and cancer. (2018) 5:. doi: 10.3389/fmed.2018.00271
WangXZhangYWangSNiHZhaoPChenGet al. The role of CXCR3 and its ligands in cancer. Front Oncol. (2022) 12:1022688. doi: 10.3389/fonc.2022.1022688
Moreno AyalaMACampbellTFZhangCDahanNBockmanAPrakashVet al. CXCR3 expression in regulatory T cells drives interactions with type I dendritic cells in tumors to restrict CD8(+) T cell antitumor immunity. Immunity. (2023) 56:1613–30.e5. doi: 10.1016/j.immuni.2023.06.003
ZagorulyaMYimLMorganDMEdwardsATorres-MejiaEMominNet al. Tissue-specific abundance of interferon-gamma drives regulatory T cells to restrain DC1-mediated priming of cytotoxic T cells against lung cancer. Immunity. (2023) 56:386–405.e10. doi: 10.1016/j.immuni.2023.01.010
LittringerKMoresiCRakebrandtNZhouXSchorerMDolowschiakTet al. Common features of regulatory T cell specialization during th1 responses. (2018) 9:. doi: 10.3389/fimmu.2018.01344
González-MartínAGómezLLustgartenJMiraEMañesS. Maximal T cell–mediated antitumor responses rely upon CCR5 expression in both CD4+ and CD8+ T cells. Cancer Res. (2011) 71:5455–66.
HatzioannouABoumpasAPapadopoulouMPapafragkosIVarveriAAlissafiTet al. Regulatory T cells in autoimmunity and cancer: A duplicitous lifestyle. Front Immunol. (2021) 12:731947. doi: 10.3389/fimmu.2021.731947
EdlundTJessellTM. Progression from extrinsic to intrinsic signaling in cell fate specification: A view from the nervous system. Cell. (1999) 96:211–24. doi: 10.1016/S0092-8674(00)80561-9
O’GarraAVieiraP. TH1 cells control themselves by producing interleukin-10. Nat Rev Immunol. (2007) 7:425–8. doi: 10.1038/nri2097
JankovicDKuglerDGSherA. IL-10 production by CD4+ effector T cells: a mechanism for self-regulation. Mucosal Immunol. (2010) 3:239–46. doi: 10.1038/mi.2010.8
TrinchieriG. Interleukin-10 production by effector T cells: Th1 cells show self control. J Exp Med. (2007) 204:239–43. doi: 10.1084/jem.20070104
CopeALe FriecGCardoneJKemperC. The Th1 life cycle: molecular control of IFN-γ to IL-10 switching. Trends Immunol. (2011) 32:278–86. doi: 10.1016/j.it.2011.03.010
HoriS. The Foxp3 interactome: a network perspective of Treg cells. Nat Immunol. (2012) 13:943–5. doi: 10.1038/ni.2424
PiersonWCauweBPolicheniASchlennerSMFranckaertDBergesJet al. Antiapoptotic Mcl-1 is critical for the survival and niche-filling capacity of Foxp3+ regulatory T cells. Nat Immunol. (2013) 14:959–65. doi: 10.1038/ni.2649
HegazyANPeineCNiesenDPanseIVainshteinYKommerCet al. Plasticity and lineage commitment of individual T(H)1 cells are determined by stable T-bet expression quantities. Sci Adv. (2024) 10:eadk2693. doi: 10.1126/sciadv.adk2693
TanS-NHaoJGeJYangYLiuLHuangJet al. Regulatory T cells converted from Th1 cells in tumors suppress cancer immunity via CD39. J Exp Med. (2025) 222:e20240445. doi: 10.1084/jem.20240445
ShiHChiH. Metabolic control of treg cell stability, plasticity, and tissue-specific heterogeneity. Front Immunol. (2019) 10:2716. doi: 10.3389/fimmu.2019.02716
WarunekJJinRMBlairSJGarisMMarzulloBWohlfertEA. Tbet Expression by Regulatory T Cells Is Needed to Protect against Th1-Mediated Immunopathology during Toxoplasma Infection in Mice. ImmunoHorizons. (2021) 5:931–43. doi: 10.4049/immunohorizons.2100080
KochMATucker-HeardGSPerdueNRKillebrewJRUrdahlKBCampbellDJ. The transcription factor T-bet controls regulatory T cell homeostasis and function during type 1 inflammation. Nat Immunol. (2009) 10:595–602. doi: 10.1038/ni.1731
SalehRElkordE. FoxP3+ T regulatory cells in cancer: Prognostic biomarkers and therapeutic targets. Cancer Letters. (2020) 490:174–85. doi: 10.1016/j.canlet.2020.07.022
SharmaASubudhiSKBlandoJScuttiJVenceLWargoJet al. Anti-CTLA-4 immunotherapy does not deplete FOXP3+ Regulatory T cells (Tregs) in human cancers. Clin Cancer Res. (2019) 25:1233–8. doi: 10.1158/1078-0432.CCR-18-0762
ThummalapalliRRicciutiBBandlamudiCMuldoonDRizviHElkriefAet al. Clinical and molecular features of long-term response to immune checkpoint inhibitors in patients with advanced non–small cell lung cancer. Clin Cancer Res. (2023) 29:4408–18. doi: 10.1158/1078-0432.CCR-23-1207
ShalataWZolnoorianJMigliozziGJamaAADudnikYCohenAYet al. Long-lasting therapeutic response following treatment with pembrolizumab in patients with non-small cell lung cancer: A real-world experience. Int J Mol Sci. (2023) 24. doi: 10.3390/ijms24065938
HeXXuC. Immune checkpoint signaling and cancer immunotherapy. Cell Res. (2020) 30:660–9. doi: 10.1038/s41422-020-0343-4
YangJBaeH. Drug conjugates for targeting regulatory T cells in the tumor microenvironment: guided missiles for cancer treatment. Exp Mol Med. (2023) 55:1996–2004. doi: 10.1038/s12276-023-01080-3
LevineAGMendozaAHemmersSMoltedoBNiecRESchizasMet al. Stability and function of regulatory T cells expressing the transcription factor T-bet. Nature. (2017) 546:421–5. doi: 10.1038/nature22360
HuoRJiangYZhangLDuSZhouD. CXCR3 inhibitors for therapeutic interventions: current status and perspectives. (2025) 16:. doi: 10.3389/fphar.2025.1556196
ZhuGYanHHPangYJianJAchyutBRLiangXet al. CXCR3 as a molecular target in breast cancer metastasis: inhibition of tumor cell migration and promotion of host anti-tumor immunity. Oncotarget. (2015) 6:43408–19. doi: 10.18632/oncotarget.6125
PradelliEKarimdjee-SoilihiBMichielsJFRicciJEMilletMAVandenbosFet al. Antagonism of chemokine receptor CXCR3 inhibits osteosarcoma metastasis to lungs. Int J cancer. (2009) 125:2586–94. doi: 10.1002/ijc.24665
JiaoHPangBChiangY-CChenQPanQRenRet al. Structure basis for the modulation of CXC chemokine receptor 3 by antagonist AMG487. Cell Discov. (2023) 9:119. doi: 10.1038/s41421-023-00617-0
BoofM-LGéhinMVoors-PetteCHsinC-HSippelVStrasserDSet al. Pharmacokinetics, pharmacodynamics and safety of the novel C-X-C chemokine receptor 3 antagonist ACT-777991: Results from the first-in-human study in healthy adults. Br J Clin Pharmacol. (2024) 90:588–99. doi: 10.1111/bcp.15914
Summary
Keywords
regulatory T cells, hybrid tregs, T-bet⁺ hTregs, GATA3, Foxp3, tumor microenvironment, immunotherapy
Citation
Azimnasab-Sorkhabi P, Soltani-asl M, Kfoury Junior JR and Ansa-Addo EA (2025) Hybrid regulatory T cells: camouflaged architects of tumor immunity. Front. Immunol. 16:1658576. doi: 10.3389/fimmu.2025.1658576
Received
02 July 2025
Accepted
03 September 2025
Published
17 September 2025
Volume
16 – 2025
Edited by
Soldevila Gloria, National Autonomous University of Mexico, Mexico
Reviewed by
Robert Bright, Texas Tech University Health Sciences Center, United States
Xinyan Wu, China Agricultural University, China
Updates
Check for updates
Copyright
© 2025 Azimnasab-Sorkhabi, Soltani-asl, Kfoury Junior and Ansa-Addo.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ephraim A. Ansa-Addo, Ephraim.ansa-addo@osumc.edu
†These authors have contributed equally to this work and share first authorship
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.





