

Losing weight doesn’t necessarily make you fitter, a new study finds.

(Photo: Oleg Breslavtsev / Getty)
Published March 25, 2026 12:36PM
Is exercise obsolete in the age of Ozempic? Now that the initial hype has settled down, nobody makes that claim with a straight face. In fact, one of the big fears among people taking GLP-1 agonists (the class of drug to which Ozempic belongs) is that they’ll lose too much muscle along with all the fat, leaving them weaker and less healthy. But at this point, there’s very little data on what happens when you combine these drugs with an exercise routine (or lack thereof).
A newly published study in the journal Sports Medicine steps into this gap. It’s a secondary analysis of data from a previously published study by researchers at the University of Copenhagen in Denmark, funded in part by the Novo Nordisk Foundation (Novo Nordisk is the company that makes Ozempic). The study follows volunteers taking another Novo Nordisk GLP-1 agonist called liraglutide (sold under the brand names Victoza and Saxenda) for an entire year, with or without the addition of a regular exercise program. The results show that without exercise, both health and physical function suffer—and it’s not just about muscle.
What the GLP-1 Study Found
The study involved 193 adults between the ages of 18 and 65. It’s a little unusual in that they started by following an eight-week very-low-calorie diet before starting either exercise or the GLP-1 drug. That’s because the original study was designed to look at ways of maintaining weight loss. Everyone included in the study lost at least 5 percent of their starting weight, which resulted in an average weight loss of 29 pounds. Then, for the following year, they either exercised, took the GLP-1 drug, did both, or did neither. (Those who didn’t get the drug got a placebo.)
The exercise program involved two group exercise classes per week, including 30 minutes of intervals on an exercise bike, then 15 minutes of circuit training (step-ups, boxing, squats, kettlebells, and so on). The subjects were also asked to do two additional workouts on their own; the details were up to them, but most chose running, cycling, brisk walking, or circuits. Adherence was decent: they averaged 2.65 workouts a week and met standard public health guidelines for physical activity.
The first outcome of interest (as reported in the original analysis) is weight. Here’s the trajectory of the four groups:
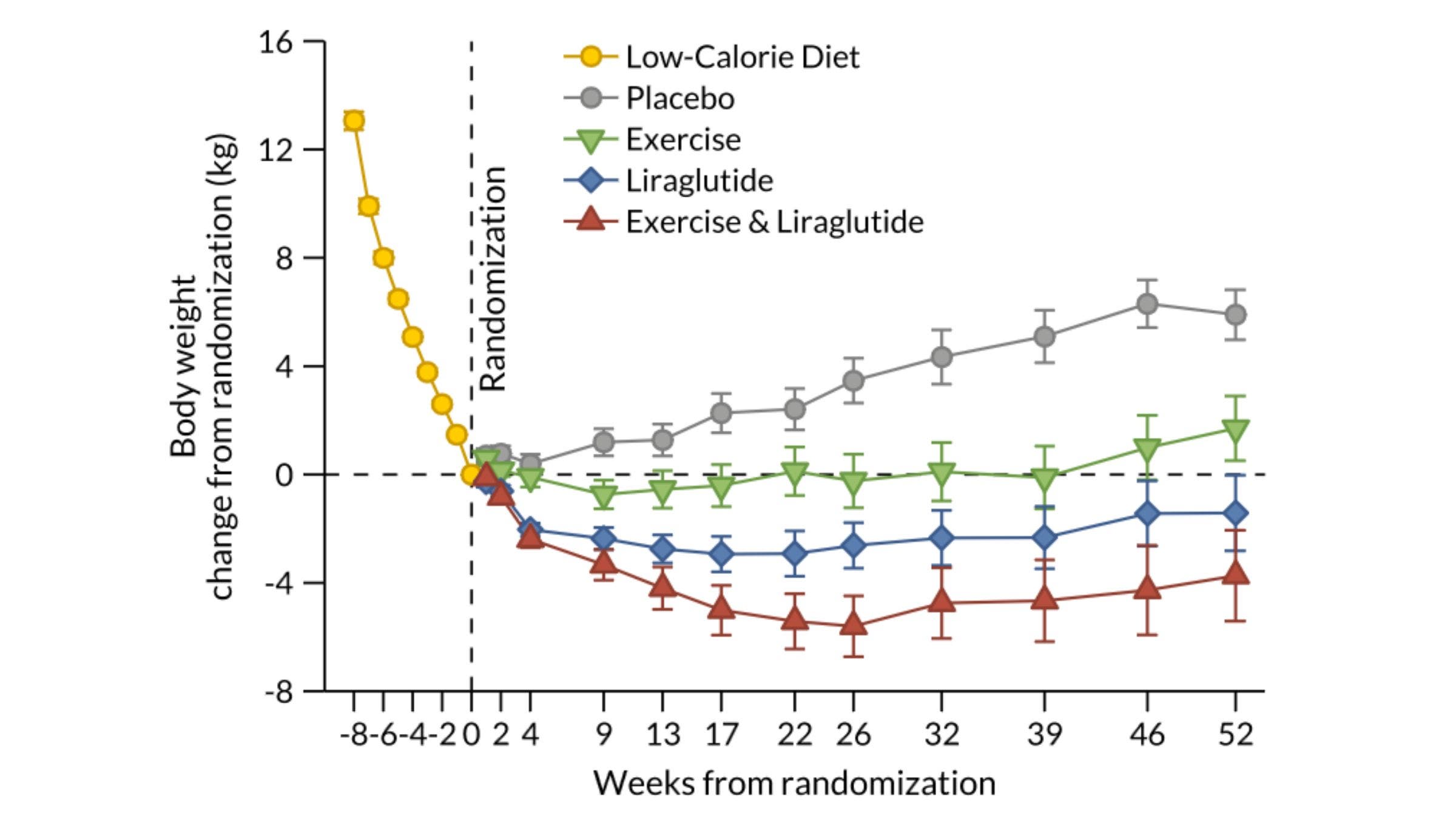 The combination of exercise and a GLP-1 drug was most effective for maintaining weight loss. (Photo: Sports Medicine)
The combination of exercise and a GLP-1 drug was most effective for maintaining weight loss. (Photo: Sports Medicine)
Doing nothing was the worst option. Exercising and taking a GLP-1 drug was the best option. If you had to choose one or the other, the drug looks marginally better, though the difference wasn’t statistically significant.
Does Fitness or Fatness Matter More?
There’s a longstanding debate about the relative health effects of being overweight versus being aerobically unfit. The two often go together, so they get conflated—but they’re not the same thing. The general trend of evidence, according to the Danish research team, is that it’s better for health and longevity to be fit and overweight than unfit and normal weight. This distinction is important in the context of GLP-1 drugs, because if they help you lose weight without gaining fitness, then the health benefits may be less than you’d expect.
Figuring out how to measure fitness in this context isn’t straightforward. When you lose weight, you’ll generally lose some muscle mass in addition to fat loss. Both strength and aerobic fitness (as measured by VO2 max) are roughly proportional to muscle mass, so your absolute fitness might appear to decline when you lose a lot of weight. But if you lose less strength or fitness in proportion to your overall weight loss, you’ll still end up with greater functional fitness: you’ll have an easier time getting up from a chair, be able to walk for longer, and so on.
One of the simple functional tests the Danish study included was a stair-climb test: climb up and down an 11-step stairway twice, as fast as possible. Here’s what those results looked like:
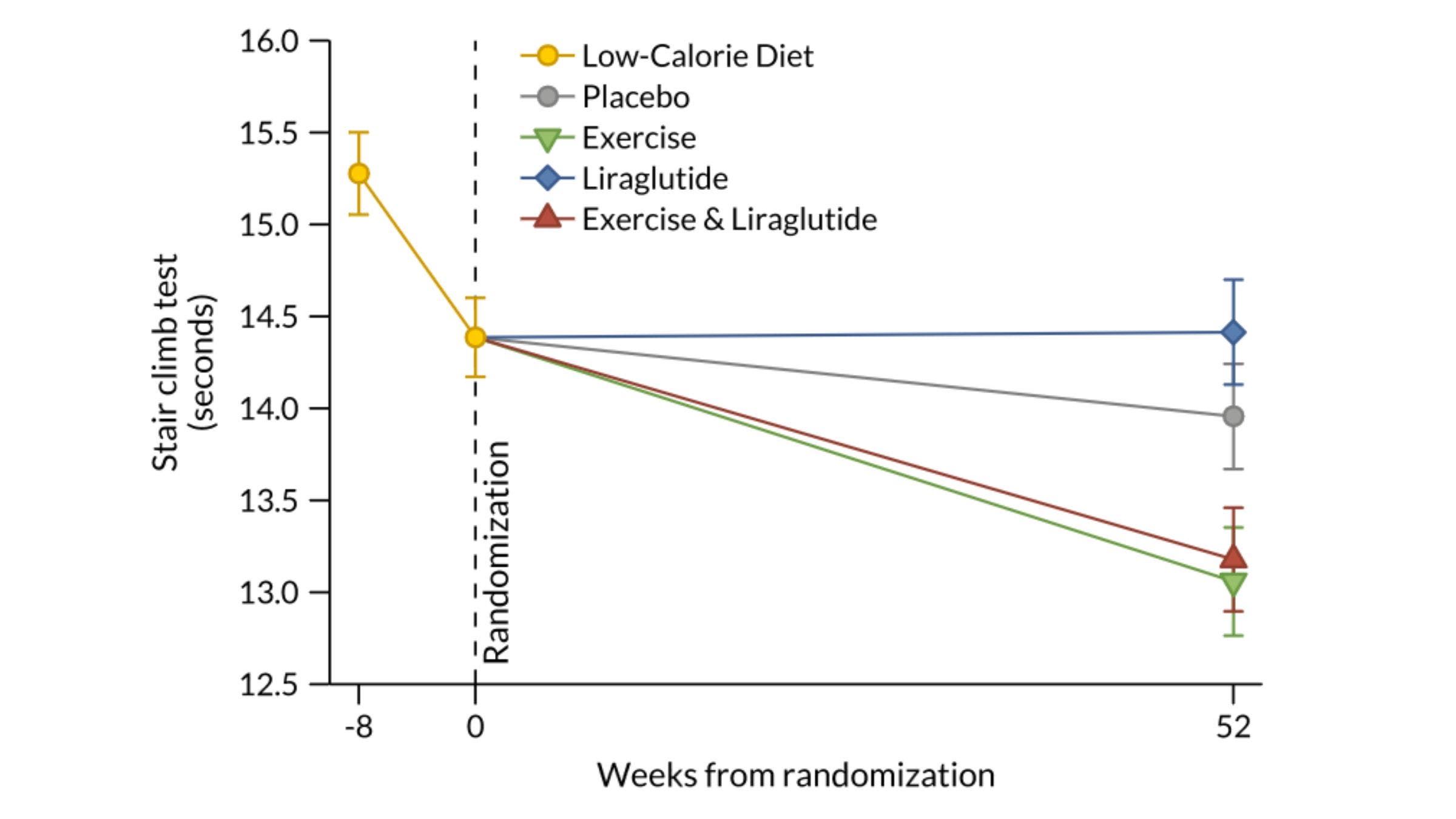 The key to climbing stairs more quickly was exercise, with or without a GLP-1 drug. (Photo: Sports Medicine)
The key to climbing stairs more quickly was exercise, with or without a GLP-1 drug. (Photo: Sports Medicine)
It’s clear here that the exercise program helped people speed up and down the stairs more quickly, whether or not they were taking the GLP-1 drug. Just taking the drug without exercising didn’t have any benefit.
There are a whole bunch of other fitness measures in the paper: VO2 max tests, leg strength tests, body composition tests to measure muscle mass in the arms and legs. The fitness outcomes can be expressed in absolute terms, or relative to total body weight, or relative to muscle mass. No matter how you express it, the overall pattern, with a few minor exceptions, is the same as the graph above: exercise makes you fitter, simply taking the drug doesn’t.
(An example of a minor exception: the drug alone was enough to improve relative leg strength, i.e. leg strength divided by total body weight, because weight decreased more than strength. But adding exercise worked even better.)
This conclusion—that the best way to get fitter is to exercise—is not exactly surprising. But I think it has been overlooked in discussions about GLP-1 drugs. I’ve certainly seen lots of chatter about the dangers of muscle loss with Ozempic, and the need to pound protein and lift weights. That’s a legitimate concern, but aerobic fitness is an even better predictor of longevity and marker of general health. GLP-1 drugs have remarkable properties, but they haven’t made exercise obsolete.
For more Sweat Science, sign up for the email newsletter and check out my new book The Explorer’s Gene: Why We Seek Big Challenges, New Flavors, and the Blank Spots on the Map.





