

What is IBS?
Irritable bowel syndrome – IBS – affects around one in ten people.
The symptoms often include abdominal pain, bloating, and diarrhoea or
constipation. However, people with IBS may also experience other symptoms, such
as headaches, muscle pain, chronic fatigue, depression, and sleep problems.
IBS is not dangerous, but it can significantly reduce a person’s quality of
life.
The causes of IBS are still not well known. There is no evidence that
psychological factors such as depression or anxiety affect the occurrence or
course of IBS. However, stress can worsen the symptoms.
There are currently no treatments that cure IBS, but several measures can
relieve the symptoms.
People with IBS may have problems digesting different types of food. They
can improve their symptoms by adjusting their diet. For example, studies have
documented that the so-called low-FODMAP diet can help.
Some feel that stress management helps.
Source: Helsenorge
There’s plenty of official advice available for people with irritable
bowel syndrome (IBS). One of them is to eat
regularly and avoid long periods without food.
But in one Norwegian professional environment, the opposite idea emerged: Maybe
the symptoms can be relieved by eating less frequently?
“We were a small group of professionals who came together as a result of
both a growing interest in intermittent fasting in the field and many anecdotes about how people who fasted experienced fewer digestive
problems,” says Marit Kolby.
She is a university lecturer and researcher at Oslo New
University College.
“But there was no research on this,” she says.
Showed improvement in most participants
In 2021, Kolby and her colleagues Asgeir Brevik and Marianne Molin began
planning a study of time-restricted eating for IBS.
This is a type of intermittent fasting where you only eat for a limited
period of the day – typically 8 hours – while you fast for the rest of the
day, i.e. 16 hours.
However, it turned out to be difficult to obtain funding for such a
study.
“One of the reasons for rejection was that this had not been researched before,” says Asgeir Brevik, an associate professor at OsloMet.
The researchers, however, believed that the lack of knowledge
was actually a very good reason to investigate the idea. So they decided to
carry out what they could without funding.
That ended up being a pilot study – a small study to pave the way for more
research.
So master’s students Maria Thompson Clausen and Henrik Sverdrup from the
University of Oslo conducted a trial with 97 patients, under the
supervision of the three researchers. The Norwegian Gastrointestinal
Association helped recruit patients.
The results showed that most participants experienced significant
improvements in symptoms.
“Could be relevant”
Gülen Arslan Lied is a professor and head of the University of Bergen’s Centre for
Nutrition, as well as a senior consultant and gastroenterologist at Haukeland University Hospital. She also researches IBS but was not involved in this study.
“You can’t say much from a pilot study. Nevertheless, this may suggest that meal timing itself – regardless of
specific food restrictions – could be relevant for the symptom burden in IBS,” she says.
“The findings may challenge the one-sided focus on what you eat and open up for the idea that when you eat may also matter,” she adds.
Lied emphasises, however, that the results must be interpreted with great
caution.
“Do not eat full meals”
Professor Bodil Ohlsson at Lund University in Sweden also studies IBS and
has published studies showing that IBS patients improved on a low-carb
diet.
She believes eating patterns may play a role.
“In dietary studies on IBS, we have seen that many patients eat small meals
all the time,” she writes in en email. “They eat irregularly and do not eat full meals; they just snack. So I
can imagine that when the stomach gets some rest at times, they feel better.”
However, Ohlsson points out that more research is needed before anything
can be said for certain.
“The weakness of this study is that it only followed patients with
time-restricted eating,” she writes. “There will always be a placebo effect when you follow
patients and give them attention. A new study with a control group that does not practice time-restricted eating is needed.”
No food restrictions
The participants in the study were individuals who reported having been diagnosed with IBS by a doctor. They practiced time-restricted eating for eight
weeks.
Participants could choose whether their eight-hour eating window should
start early or late in the day. It was also possible to adjust the timing somewhat – for example, if they had a late dinner – as long as the fasting period lasted at least 16 hours.
Otherwise, there were no restrictions on what or how much the participants
ate. They were encouraged to eat until full at meals and maintain the same
weight.
The participants kept in contact with the researchers and with each other in a closed
Facebook group.
Both before and after the eight weeks, the participants answered an
IBS-SSS questionnaire, which is designed to assess IBS symptoms.
The results showed substantial improvement in many participants.
IBS-SSS – a measure of IBS
This questionnaire contains questions about pain, bloating, bowel
movements, and how much IBS symptoms affect a person’s life. A score between 0
and 500 is calculated based on the answers. The more symptoms a person has, the
higher the score.
0-74 points = no IBS
75-174 points = mild IBS
175-300 points = moderate IBS
301-500 points = severe IBS
Made a difference
“We were very excited before conducting the first analyses,” says
Clausen.
It then became clear that the IBS-SSS score decreased by an average of 100
points from the beginning to the end of the experiment. This is double what is
considered clinically relevant – meaning an effect large enough to make
a difference for the patient.
But the results were not the same for everyone.
“We saw the best results in those who had IBS with constipation,” says
Clausen.
There were also significant differences between participants.
Many got better – some got worse
“We also looked at what happened to each individual participant. That was
very interesting,” Clausen says.
This overview showed that most people improved after fasting. By the end
of the study, there were clearly fewer people with severe IBS. Some participants had improved a great deal. 12 participants no longer had
IBS symptoms.
On the other hand, a few patients became worse. A couple became much worse.
Based on the data in the study, it’s not possible to say why. For example, the
researchers do not know whether some of the participants followed the regimen more closely than others.
Kolby believes that the variation suggests a need for individualised treatment.
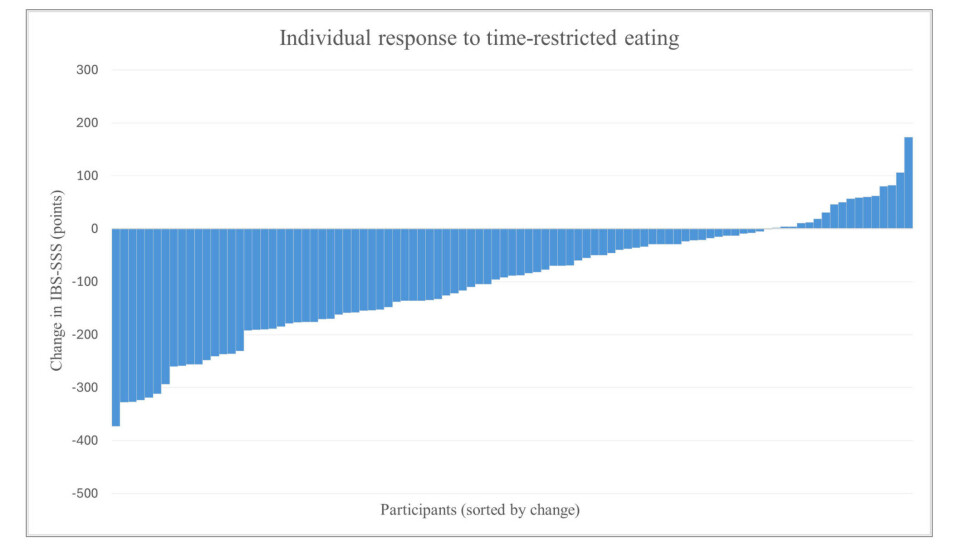
Each of the blue bars represents a patient. The length of the bars shows how big the change in IBS symptoms was from the beginning to the end of the study. The more the bar is below the zero (base) line, the fewer IBS symptoms the patient has. Bars that extend above the zero line represent patients who got worse.
(Graph: Clausen et al., 2026)
Large variations among patients
Lied from the University of Bergen also believes that patients need individually tailored IBS
treatment.
“We know from IBS in general that there are large variations among patients,”
she says.
IBS can, for example, have different underlying causes. This and many
other factors can have an impact on the effect of time-restricted eating, Lied
believes.
“Differences in circadian rhythm, stress response, timing of the eating window,
food intake, and psychosocial factors may play a role. And, not least, for some
people fasting itself can be a stress factor that worsens symptoms,” she says.
Several possible mechanisms
The pilot study cannot tell us anything about why time-restricted eating
may alleviate symptoms in people with IBS.
However, Kolby and her colleagues still have some ideas about about which biological mechanisms may be involved.

Gülen Arslan Lied is a professor and head of the Centre for Nutrition at the University of Bergen, as well as a senior consultant and gastroenterologist at Haukeland University Hospital.
(Photo: University of Bergen)
It is, for example, known that fasting stimulates the so-called migrating
motor complex – muscle movements that help clear the small intestine of
bacteria and food residues. Fasting is also associated with less inflammation in the body.
Many hours without food may also change the composition of intestinal
bacteria. It can also cause the body to switch to using fat as an energy source
and become more efficient at removing cells that are not functioning properly.
“Larger studies are needed”
“Several of these mechanisms overlap with known pathophysiological
features of IBS, but the study did not measure any biological markers or
mechanisms,” says Lied.
“We still lack scientific evidence. Time-restricted eating should
therefore not be seen as a replacement for existing treatment. Larger
randomised, placebo-controlled studies are needed to determine whether it was really
the fasting that led to the improvement,” she adds.
Ohlsson from Lund University believes we should work towards helping patients develop regular eating habits with full meals.
“You can start there. Then fasting can be evaluated further through more studies. Since there is a connection between eating disorders and IBS, it’s important not to introduce measures that could trigger eating disorders,” she writes.
Significant symptoms
Kolby hopes the results from the pilot will make it easier to get funding
for larger studies.
“A recent Norwegian study showed that many IBS sufferers have significant symptoms and do not feel that they are receiving enough help from the healthcare system,” she says.
Time-restricted eating is free, quite easy to implement, and places no restrictions on what food you can eat. If it proves effective, this eating
pattern could become a new tool in the IBS treatment toolbox.
Too little research funding
Previous studies have also shown that both low-carb diets and the
Mediterranean diet can relieve IBS symptoms. There is also some evidence that
the condition is linked to ultra-processed foods.
In 2022, Kolby published a book about fasting and whole food-based diets.
However, she says that there are no financial interests behind her desire
to study how eating patterns can affect IBS.
Kolby explains that the research group has been expanded, with Jørgen Valeur
and Hanna Fjeldheim Dale from Lovisenberg Diaconal Hospital. They are currently applying for funding to test the effect of a combination of a whole food-based diet and
time-restricted eating on IBS.
Perhaps the results from the pilot study could help in the competition for funding.
Marianne Molin, professor at Kristiania University College, believes there is far too little research funding available in this field.
“It’s a problem that there’s not more public funding to investigate a
health issue that affects so many people,” she says.
References:
Clausen et el. Time-Restricted Eating and Symptom Severity in Irritable
Bowel Syndrome: Results from a Pilot Study, Nutrients, 2026. DOI: 10.3390/nu18050765
Dale et al. Ultra-Processed Food Consumption and Irritable Bowel Syndrome: Current Evidence and Clinical Implications, Nutrients, 2025. DOI: 10.3390/nu17223567
El-Salhy et al. Quality of life, functional impairment and healthcare experiences of patients with irritable bowel syndrome in Norway: an online survey, BMC Gastroenterology, 2025. DOI: 10.1186/s12876-025-03685-6
Nilholm et al. Assessment of a 4-Week Starch- and Sucrose-Reduced Diet and Its Effects on Gastrointestinal Symptoms and Inflammatory Parameters among Patients with Irritable Bowel Syndrome, Nutrients, 2021. DOI: 10.3390/nu13020416
———
Translated by Nancy Bazilchuk
Subscribe to our newsletter
The latest news from Science Norway, sent twice a week and completely free.





