

Study design
This study adopted a 2 (time: pre-test, post-test) × 2 (group: experimental group, control group) mixed experimental design, with time as the within-subjects factor and group as the between-subjects factor. The study was conducted between June and September 2025 in Foshan City, Guangdong Province, China. The study protocol received approval from the Ethics Committee of Guangzhou Sport University (Approval No.: 2025LCLL-067) and was registered with the Chinese Clinical Trial Registry (Registration No.: CTR2500103810). This investigation was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all parents/legal guardians of the participants prior to their inclusion in the study.
Participants and grouping
A total of 23 children with autism were initially recruited from the third grade of Foshan Qizhi School. Based on the inclusion and exclusion criteria(Table 1), 20 participants met the eligibility requirements and were included in the study. They were assigned to either the experimental group (n = 10) or the control group (n = 10), matched according to demographic variables such as age, sex, and class. The experimental group received a combined Physical Activity and Educational Drama intervention, while the control group participated in a conventional Physical Activity intervention. Participants were informed that they could withdraw from the study at any time without penalty if they experienced discomfort or were unwilling to continue during the intervention period. All 20 participants completed the entire intervention with no missing data(Figure 1).
Table 1 Inclusion and exclusion criteria of the study participants.Fig. 1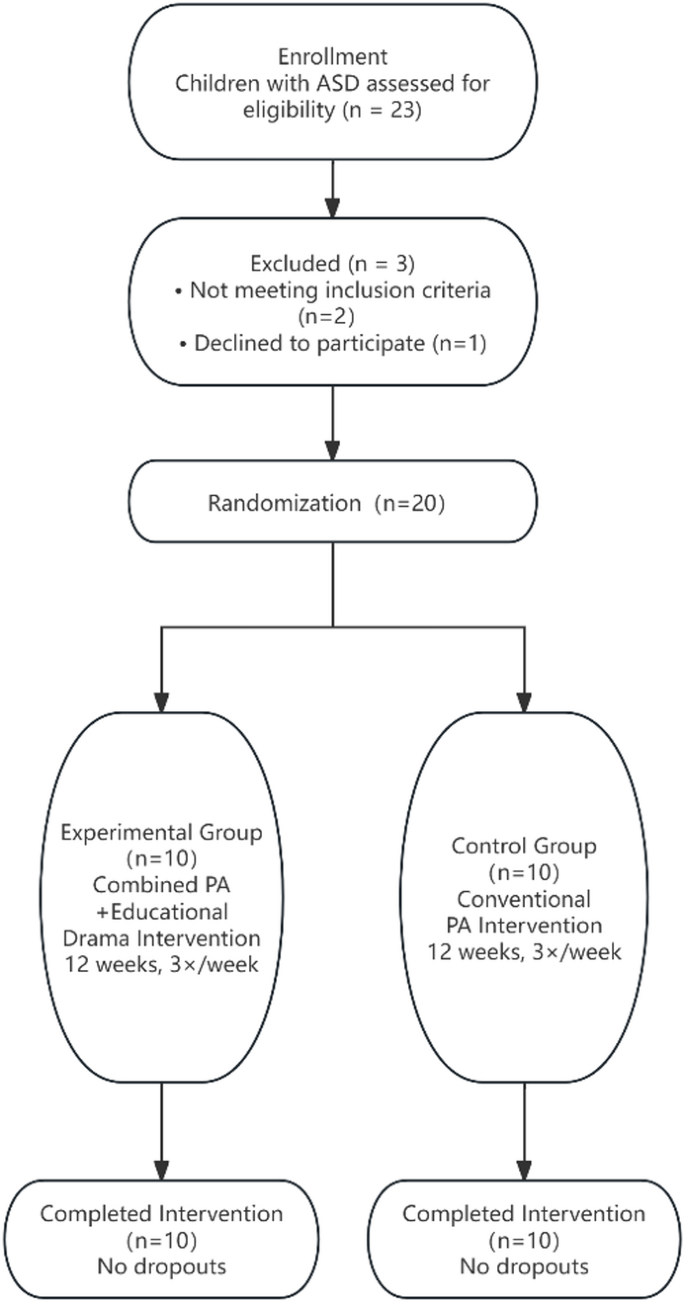
Recruitment flow diagram.
Randomization
Numbers (1–20) were assigned to the participants according to their recruitment times in an Excel software database, and a random sequence was then generated using the “= rand()” formula. This sequence was sorted to allocate the participants to the study groups. These tasks were completed by professional computer workers blinded to recruitment and allocation after the recruitment process had concluded.
Experimental group
The Physical Activity combined with Educational Drama intervention consisted of three progressive stages: adaptation, fundamental, and advanced phases (Table 2). Each session followed a structured sequence comprising a warm-up, foundational training, core activity, and relaxation segment ( Table 3). The intervention dosage was as follows: (1) each session lasted 30 min; (2) exercise intensity was maintained at a moderate level, corresponding to 60–69% of the participant’s maximum heart rate (maximum heart rate = 220-age); (3) the intervention period lasted 12 weeks(2025.6.15-2025.9.10); and (4) sessions were conducted three times per week.
Table 2 The combined physical exercise and educational drama intervention program.Table 3 Introduction to educational drama warm-up activities.
The intervention was primarily delivered by graduate students majoring in Physical Education who held official teaching qualifications. Instruction was conducted in group sessions. Given that children with autism often have difficulty participating independently, their guardians were encouraged to accompany them during the sessions. To ensure consistent attendance and maximize the effectiveness of the intervention, strict attendance records were maintained for each class; participants were not permitted to miss more than three consecutive sessions or more than seven sessions in total. In addition, during each session, two children with autism were randomly selected to wear Polar heart rate monitors to assess exercise intensity. Across the 12-week intervention period, the mean heart rate of the experimental group was 136.21 ± 6.19 beats/min, corresponding to a moderate-intensity level. The specific content and curriculum structure of the experimental group are presented in Tables 4 and 5.
Table 4 Drama picture book.Table 5 Curriculum structure for the experimental group.Control group
The control group intervention followed a structured program consisting of three progressive stages: adaptation, fundamental, and advanced phases (Table 6). Each session included a warm-up, foundational training, core activity, and relaxation segment (Table 7). The dosage, intensity, and frequency of the intervention protocol were maintained consistent with those of the experimental group, while being devoid of any educational drama components. The sessions were primarily conducted by graduate students majoring in Physical Education who held official teaching qualifications, using a group-based instructional format. The control group used the same Polar heart rate monitors as the experimental group to collect participants’ heart rate data. Across the 12-week intervention period, the mean heart rate of the control group was 135.43 ± 8.37 beats/min, corresponding to a moderate-intensity level parents did not participate in the intervention process of either group and were instructed to avoid providing active guidance or prompting to the children.
Table 6 Intervention protocol for the control group.Table 7 Curriculum structure for the control group.Measurement of core symptoms
The pre-test was conducted within one week prior to the intervention, and the post-test was completed within one week following the 12-week intervention period.
Repetitive behaviors
The Repetitive Behavior Scale–Revised (RBS-R) is a validated instrument for assessing stereotyped behaviors in children with autism18,19. The scale comprises 43 items across six subdomains: stereotyped behavior, self-injurious behavior, compulsive behavior, ritualistic behavior, sameness behavior, and restricted behavior. Items are rated on a 4-point scale, where 3 indicates severe behavioral problems, 2 indicates moderate problems, 1 indicates mild problems, and 0 indicates no problems. Higher scores reflect greater severity of repetitive and stereotyped behaviors. The scale was completed by guardians based on the child’s typical behavior in daily life over the past three months, with the same informant completing it at all assessment time points and being blind to group assignment.
The social responsiveness scale, second edition (SRS-2)
Social responsiveness was assessed using the Social Responsiveness Scale, Second Edition (SRS-2)19,20. The 65-item instrument comprises five subscales: Social Awareness, Social Cognition, Social Communication, Social Motivation, and Restricted Interests and Repetitive Behaviors. Items are rated on a 4-point Likert scale, where 3 indicates severe behavioral problems, 2 moderate problems, 1 mild problems, and 0 indicates no observable behavioral problems. Higher total scores reflect more severe social impairment. The scale was completed by guardians based on the child’s typical behavior in daily life over the past three months, with the same informant completing it at all assessment time points and being blind to group assignment.
Childhood autism rating scale (CARS)
The Childhood Autism Rating Scale (CARS) (Schopler et al., 1980) was administered at baseline only. The total scores range from 0 to 60, with the following clinical cutoffs: a score below 30 indicates a non-autistic classification; a score of 30 or above leads to an autism classification. Within the autism spectrum, scores of 30–37 are classified as mild-to-moderate autism, while scores ranging from 37 to 60, accompanied by at least five items rated above 3, are classified as severe autism21.
Measurement of basic physical fitness
Based on the school’s physical fitness testing schedule and the content of fundamental movement skill assessment scales, the basic physical fitness test battery was determined to comprise the following items: standing long jump, tennis ball throw, balance beam walk, shuttle run, and two-foot continuous jump. Both the pre-test (administered within one week before the intervention) and the post-test (conducted within one week after the 12-week intervention) were carried out in close proximity to the respective start and end of the intervention period.
Standing long jump
The participant stood behind the take-off line with feet naturally apart, assumed a semi-squat position, and swung the arms backward with appropriate flexion. Subsequently, the arms were swung forward forcefully while the feet pushed off the ground to jump forward as far as possible. Two trials were performed, and the better result was recorded.
Tennis ball throw
Facing the throwing direction, the participant stood approximately one step behind the throwing line with feet in a staggered stance. Holding a tennis ball with one hand overhead, the participant threw it forward as far as possible. A forward step with the rear foot was permitted during the release, but neither foot could touch or cross the throwing line.
Balance beam walk
The balance beam was 15 cm in height, 3 m in length, and 20 cm in width. Starting from a platform behind the “start line” of the beam, the participant stood with arms abducted to the side and then walked forward by alternating steps. Test personnel walked alongside the beam to observe performance and prevent accidents. Timing stopped when either foot contacted the “end line.”
Shuttle run
Beginning in a standing start position, timing commenced upon a verbal signal. The participant ran to a turn-around point, touched a designated object, turned, and ran back to the finish line, at which point timing was stopped. The total running distance was 10 m.
Two-foot continuous jump
Ten soft blocks were placed in a straight line on level ground at 50 cm intervals. A “start line” was marked 20 cm from the first block, and a “finish line” was marked 20 cm beyond the last block. With feet together behind the start line, the participant performed a two-footed jump consecutively over all ten blocks without stopping.
All physical fitness tests were administered by two fixed research assistants with backgrounds in sports measurement. Prior to data collection, they underwent a week of standardized training. Both assessors remained blind to the participants’ group assignments.
Statistical analysis
All statistical analyses were performed using SPSS (Version 27.0). The normality of continuous variables was assessed using the Shapiro‑Wilk test, and descriptive statistics are presented as mean ± standard deviation. For data conforming to a normal distribution, independent samples t‑tests were used to examine baseline differences between the two groups. Otherwise, the Mann-Whitney U test was employed. Categorical variables were compared using the chi-square test. A two‑way repeated‑measures analysis of variance (ANOVA) was then conducted, with group (intervention vs. control) as the between‑subjects factor and time (pre‑intervention vs. post‑intervention) as the within‑subjects factor. The Bonferroni correction was applied for post‑hoc comparisons, and the Greenhouse‑Geisser correction was used when the assumption of sphericity was violated. In cases of a significant interaction effect, simple effect analyses were performed. A p‑value < 0.05 was considered statistically significant.





