




To our knowledge, this study is the first attempt to demonstrate an association between serum thyroid hormone, ferritin, folic acid, vitamin B12 levels and the risk of pterygium in human population-based study. The cause of pterygium remains unknown despite numerous investigations. The following have been proposed as risk factors: oxidative stress, viral involvement, ocular surface alterations, genetics, ultraviolet radiation (UVR), viral inheritance, and environmental variables9. Our results suggest that subjects with high total serum T3 tend to have a significantly increased risk of developing pterygium. The association between serum thyroid hormones and pterygium is not fully understood. One of the possible reasons for the higher serum T3 levels in pterygium patients compared to the control group may be that thyroid hormones, including T3, play a role in many physiological processes such as cell proliferation, metabolism and inflammation. Although there are no studies on the relationship between high serum thyroid hormones and pterygium, this result may be possible in pterygium where chronic inflammation is thought to be predominant. In addition, research has shown that thyroid hormones may regulate the antioxidant defense system. For example, they can increase the expression and activity of antioxidant enzymes such as superoxide dismutase (SOD) and catalase, which play important roles in reducing oxidative stress10. This protective effect supports the finding of high T3 values in the development of pterygium in which oxidative stress is blamed.
Other possible causes include proptotic appearance due to thyroid hormones and higher exposure to UV radiation due to lid retractions. This assumption is actually a statement of summary inference from the literature. In their study, Ozer et al.11 found that the prevalence of pingeacula formation, which is accepted to have a similar pathophysiology with pterygium, was higher in patients with thyroid orbitopathy compared to the control group.
Angiogenesis, cell proliferation, tissue invasion, and inflammation are all important factors in the production of pterygiums, as demonstrated by a recent study that found that pterygium epithelial cell cultures exposed to UVR release pro-inflammatory cytokines like interleukin IL-6 and IL-812. The use of topical vitamin D (VD) has also been demonstrated to suppress ocular surface inflammation and corneal neovascularization by preventing the migration of Langerhans cells from the conjunctiva to the cornea and the release of IL-1a, IL-1b, IL-6, and IL-8 by corneal epithelial cells respectively.13 While 25(OH)D(D3) is the predominant form of VD in the circulatory system, 1,25(OH)(D2) is the active intracellular binding form. Serum 25(OH)D levels are used to determine the state of VD14. Season, skin pigmentation, age, sex, and obesity are risk factors for vitamin D insufficiency8. Age, sex, and BMI of the groups in our study were comparable (p < 0.05). It can be expressed as an indicator that there is a balanced distribution between groups. The same amount of time was used to gather the blood samples. The fact that vitamin D levels were lower in patients with pterygium compared to the control group in our study supports the presence of anti-inflammatory effect of vitamin D in pterygium, which is accepted to develop due to chronic inflammation, and may mean that inadequate protection from inflammation may be effective in the development of pterygium.
The inflammatory response and wound healing process in pterygium are clearly dysregulated. This was supported by a study on pterygium tissue. In this study, it was accepted that acute inflammation could not be controlled due to disruption of the oxidant-antioxidant balance; the HO1-HO2 expression ratio was disrupted, and the event turned into chronic inflammation.15 Exposure to UVA and UVB is linked to photochemical cell damage. Lipid peroxidation, a reduction in mitochondrial viability, and direct damage to DNA are examples of this damage. By breaking down ferritin, UV-A radiation increases the amount of free iron that is immediately detectably present in the cytoplasm of human skin fibroblasts and keratinocytes. It also reduces the binding activity of iron regulatory protein 1 (IRP-1)16 The Fenton reaction uses the freed iron to catalyze the production of ROS caused by UV radiation17. The iron-scavenging action of ferritin is primarily responsible for maintaining the low level of intracellular free iron concentration, which is generally strictly regulated. Ferritin, which was previously believed to be restricted to the cytoplasm, has been discovered in the avian corneal epithelium’s nuclei and may protect DNA from UV-induced free radical damage.18 In the study conducted by Fox et al.16 on pterygium tissue, ferritin mRNA levels were found to be 3 times lower in pterygium compared to controls, suggesting that ferritin plays a role in the pro-oxidant and inflammatory status of pterygium tissue. Although pterygium is thought to be a local pathology in our study, the fact that serum ferritin levels were significantly lower in the pterygium group compared to the control group supports that the anti-inflammatory mechanism deficiency is also affected systemically. This may be related to the severity of the condition in the cornea, and in this regard, it may be useful to compare cellular and tissue samples with serum values.
Vitamin B12 is a water-soluble vitamin that is essential for the proper functioning of the human body. The main rationale for evaluating vitamin B12 levels in this study was to understand whether there is a change in vitamin B12 levels in the pathogenesis of pterygium, a fibrovascular inflammation. There is insufficient data to support the hypothesis that vitamin B12 levels and inflammation are directly correlated. In a large population-based investigation, Young et al.19 found a comparable association between vitamin B12 level and C-reactive protein (CRP) for some races, whereas Al-Daghri et al.20 observed a substantial negative link between vitamin B12 level and tumor necrosis factor-α (TNF-α). Studies conducted on experimental animals have demonstrated that a deficit in vitamin B12 initiates proinflammatory pathways via interleukin-10 (IL-10), monocyte chemoattractant protein-1 (MCP-1), and interleukin-1β (IL-1β)21. However, opinions differ about the mechanism and potential severity of the body’s inflammation caused by a vitamin B12 shortage.
A vitamin B12 shortage can lead to mucocutaneous illnesses such as vitiligo, aphthous stomatitis, and atopic dermatitis22. Serum vitamin B12 levels in pterygium have never been studied, as far as we are aware. In this study, serum vitamin B12 levels were significantly lower in pterygium patients than in controls, and gender had no effect on the outcomes. The large sample size enhanced the conclusion’s strong statistical power. This result can be interpreted in two ways: (1) By causing inflammatory processes in the corneal and conjunctival tissue, low vitamin B12 levels may have a role in the pathophysiology of certain disorders. Recent studies have shown a connection between low vitamin B12 levels and inflammation in a number of organs, including the liver, gut, and bone.23 It’s not clear enough right now, though, therefore additional future experimental work is required to clarify the exact mechanism. (2) In the same general systemic inflammatory disease, pterygium and low vitamin B12 levels may be independent results. Given that pterygium or low vitamin B12 levels are known to be linked to some systemic disorders, this theory may also be deemed plausible.In those with a systemic illness brought on by low vitamin B12 levels, pterygium and related ophthalmologic disorders may go unnoticed9,21.This may help to clarify the association. Physicians who are keeping an eye on the patient should ask about any ocular surface complaints and seek consultation from an ophthalmologist as needed.
According to Bresscoll et al.22, vitamin B12 may be utilized therapeutically to treat a few mucocutaneous conditions. Based on the findings of this investigation, it is plausible that elevated levels of vitamin B12 may serve as a preventive measure or a therapeutic approach for pterygium. However, given the number of documented side effects from vitamin B12 supplementation and the need for more prospective randomized trials to confirm its efficacy and safety, this is currently a very compelling argument19.
Like vitamin B12, folic acid is a water-soluble vitamin that the body is unable to produce on its own and must get from food or supplements24. Serum folic acid levels in pterygium have never been studied, as far as we are aware. The study’s findings indicate that, in comparison to healthy controls, pterygium patients had decreased serum folic acid levels. This result can be interpreted as follows; (1) There is limited evidence of the presence of a direct association between vitamin folic acid level and inflammation. Supplementing with vitamin B12 and folate through food may have therapeutic potential to prevent or treat nonalcoholic steatohepatitis, according to research done on mice, primates, and people. Our results are consistent with the literature, and the inflammatory nature of pterygium is supported by the fact that folic acid can be utilized to prevent the known inflammatory condition nonalcoholic steatohepatitis. (2) Given our similar interpretation of vitamin B12, it is also possible that low folic acid levels and pterygium are distinct outcomes described in the same broad systemic inflammatory illness. Given the documented associations between pterygium and low folic acid levels and various systemic disorders, this explanation may have some merit.
The study has also some important limitations. Firstly, the subjects were selected from a single center, which can cause a selection bias. Generally, the incidence of ptrygium is influenced by genetic background25. In addition, further research should be conducted on the systemic inflammatory status of patients with recurrent pterygium. Only patients with primary pterygium were included in our study. The clinical classification of pterygium according to TAN was evaluated according to lesion size, corneal invasion, optic zone involvement and vascularization and was noted by the same physician (FS). Comparison between subgroups could not be made because there were not enough people to make a statistical difference between the groups, which is another limitation of this study. Another limitation was that we did not use additional biomarkers to assess systemic inflammatory cytokines and did not perform histopathological examinations. These are much more costly than biochemical tests but provide similarly reliable results. There are studies suggesting that high neutrophil-to-lymphocyte ratios (NLR) may serve as a biomarker for systemic inflammation in pterygium patients and that systemic inflammatory processes may contribute to the local inflammatory environment on the ocular surface.(26) Another limitation of our study is that NLR values were not examined in our study and it was not investigated whether they supported the factors examined. Comparisons between subgroups with a larger number of patients will provide valuable information to the literature as the subject of future studies.
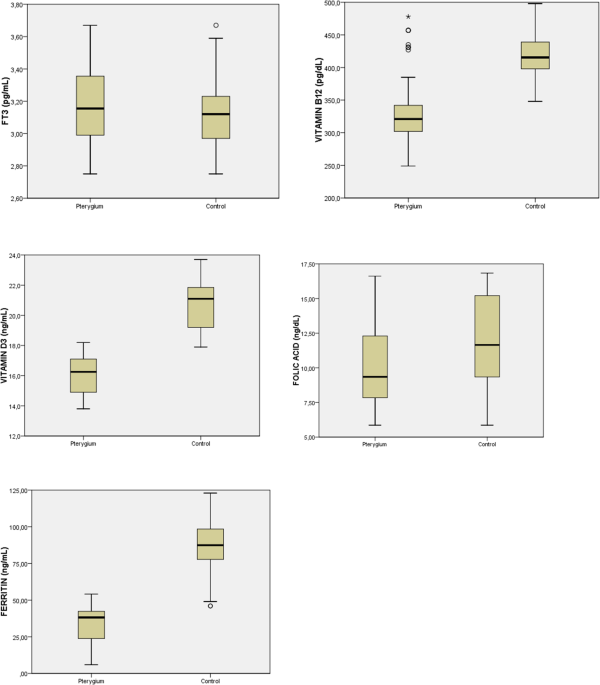
In conclusion, this study reports that pterygium patients have lower serum vitamin B12, folic acid, ferritin and vitamin D3 levels than healthy individuals. Further histological prospective studies should be designed to clarify the relationship between vitamin B12 and vitamin D3 levels and pterygium pathophysiology and the feasibility of vitamin B12 and vitamin D3 supplementation for treatment or prevention of recurrence. This may be the subject of a new study.